Obesity can mimic asthma, it affects respiratory symptoms and lung mechanics, but it can also overlap of course. Asthma is more often diagnosed in obese (misdiagnosed?). Maternal obesity (and gestational weight gain) in pregnancy. Each BMI increase of 1kg/m2 increases risk by 2-3%!
Obesity is one of the factors associated with fatal asthma attacks (but note socioeconomic confounding).
Weight reduction leads to improved lung function, health status, symptoms and morbidity in adults. Not yet proven in adolescents.
Slightly increased risk of acute asthma attacks in obese adults and school age children.
One of the Herpes virus family, and like other herpesviruses (herpes, varicella) becomes latent in the body after infection, in the case of EBV in B-lymphocytes. Immune system has developed specific strategies over the course of human evolution to control it – hence specific immunodeficiencies such as Duncan’s syndrome where EBV appears to be the only infection that becomes problematic (even catastrophic).
Associated with a number of tumours, including non-Hodgkin’s lymphoma, Burkitt Lymphoma (especially in Africa), nasopharyngeal carcinoma.
In most children, a mild febrile illness, with lymphadenopathy (“glandular fever” or infectious mononucleosis), sore throat (can be severe). Failure to improve with antibiotics is a clue! Peak age for severe presentations is teenagers – “kissing disease” (sexually transmitted!? Edinburgh students study found lower rates if routine barrier methods used). Prolonged incubation period of 30-50 days!
Classically rash triggered by amoxicillin (which is why amoxicillin isn’t recommended for sore throats, but rash can be seen with penicillin too) – maculopapular, sometimes petechial and/or urticarial, which is rather more suggestive.
On examination, hepatosplenomegaly can be seen.
Diagnosis
Blood film characteristically shows atypical lymphocytosis. Monospot test (for “heterophile” antibodies, against horse blood cells, characteristic of EBV) only 70-90% sensitive, even worse under 4yrs of age. May also be negative if done too early. Also prone to false positives although this is rare (lymphoma, hepatitis).
Serology is a bit complicated – anti VCA (viral capsid antigen) IgM comes up first, IgG follows after 2-4 weeks then persists for life. Anti EA (early antigen) IgG is an unusual one which comes up quickly and then disappears after 3-6 months. EBNA (ENV nuclear antigen) only comes up after a few months. There are false negatives (usually because illness resolves before any antibodies appear) and false positives.
If important to know, do PCR.
Mild hepatitis and cholestasis pretty common. So can be confused with autoimmune hepatitis, especially since both can give positive IM tests.
Rarer features are dacrocystitis, pneumonia, myocarditis, low platelets and neutrophils, interstitial nephritis, encephalitis. Haemophagocytic syndrome. 20x higher risk of Guillain Barre syndrome after EBV.
Splenic rupture after EBV has been reported but is very rare. Advice usually given to avoid contact sports. In ultrasound studies, peak spleen size is typically noted within the first 2 weeks of illness, but may extend to 3.5 weeks. The majority of spleen injuries occur within the first 21 days of illness and are exceedingly rare at >28 days, so one month avoidance probably sufficient.
=allergic rhinoconjunctivitis due to seasonal triggers, typically grass and/or tree pollen, can also be weeds/moulds. First described by John Bostock in 1819, so a new disease!?
More likely if born in early months of year!?
So itchy, swollen, watery eyes, runny and/or blocked nose, sneezing. Often itchy throat and ears too. Cobble stone appearance can be seen at the back of throat.
Not dangerous, but can seriously affect quality of life: poor sleep, poor concentration (exams usually at worst time of year), embarrassment about snot. One study in England showed that children with hay fever requiring anti-histamines are significantly more likely (43%) not to achieve predicted exam grades, especially when using first generation sedating antihistamines such as Piriton (chlorphenamine) [Samantha Walker, JACI 2007: 120; 381-387].
Associated with other atopic conditions, such as food allergy and asthma. Moderate to severe hay fever also associated with worse, uncontrolled asthma. London study found hospital admissions for asthma 50% higher 3 days after high grass pollen levels (inconclusive for tree pollen). [Int J Biometeorol. 2017]Brussels study found similar, compounded by air pollution. Treatment of hay fever with intranasal steroids or class 2 antihistamines reduced admissions by up to 80%. [asthma res and pract2015]
Pollen is too large to trigger the lower airways directly, rather, pollen exposure in the upper airways trigger inflammation that travels down (probably over a period of weeks) to the lower airways. An exception is when pollen grains are fragmented, as seen in thunder storm asthma where one night in Melbourne, 2016, several thousand acute respiratory presentations came to ED (up over 600%), asthma admissions up over 900%, hospitals ran out of inhalers. 10 deaths implicated. [Australia, Clin Exp Allergy. 2018;48:1421‐1428]. Complex though, rain/moisture probably contribute to pollen grain rupture, and atmospherics bring surges of pollen down to ground level.
There are many different species of grass, but if allergic to one you tend to be allergic to all of them. Trees on the other hand vary, you tend to be allergic to specific groups of trees. In Europe the most important are birch (northern Europe) and olive (Southern Europe). Birch pollen cross reacts with alder, hazel, hornbeam, beech, oak, chestnut. Olive is related to ash and lilac, cross reacts to a degree with birch. Cedar and cypress are related, pine (spruce/fir etc) are different but latter pollens are heavier and thought not to be as relevant to symptoms. Weeds belong to various unrelated families.
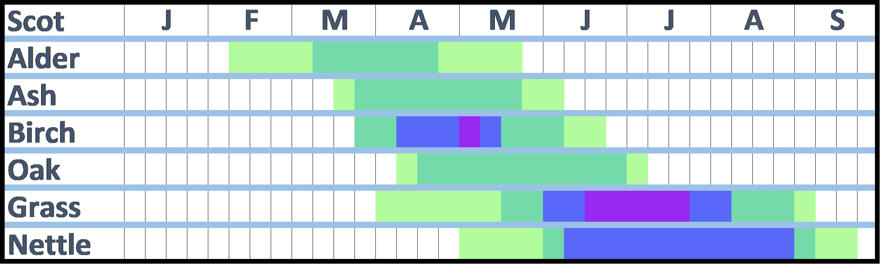
Hazel trees can start producing pollen in January! Peak is Feb/March. Alder is next earliest (see chart below). Pine is quite late, similar to grass. Weeds such as nettle can continue producing pollen through September! Cypress blooms in winter!
Average start of grass season in Scotland is mid-May (dark green on chart below), high counts generally start 1st week of June (blue), peak (purple) is mid-June to mid-July. (Light green is earliest/latest appearance, low risk).
Average start of birch season in Scotland is last week in March, highest counts end April, early May.
It’s not just pollen count – the amount of allergen carried by the pollen (“pollen potency“) varies too. Correlates pretty closely but varies by time and place, 4-5 fold difference geographically (especially grass). France has the highest yearly average grass pollen potency, 7-fold higher than Portugal. Olive pollen from two locations 400km apart varied 4-fold in their allergen potency – in Portugal there are times when pollen from Spain probably more of a problem for triggering hay fever than pollen from “local” trees! [Health Impacts of Airborne Allergen Information Network (HIALINE project)]
Moulds seem more associated with asthma than hay fever.
Management
Watch the pollen count, and choose activities inside or outside accordingly. There are apps that can help with this. But note that the time of day is important too – for grass pollen, the risk is greatest in the first half of the morning and again from about 4pm in the afternoon, until late evening. But can persist into the early hours if temperatures remain high, this effect is particularly noticeable in the cities of the south of England. For tree pollen, the risk is usually during daylight hours only.
Closing windows, or at least not sitting near windows should help. Wash your hair more regularly. Don’t dry clothes outside. Pollen barrier balms available (evidence?). Big, wrap around sunglasses?
Air purifiers with a HEPA filter should help but doors and windows will need to be closed. Unfortunately the best ones tend to be big, expensive and noisy, and price does not mean good quality. Plus you have to remember to replace the filters. The cheapest Which? recommended one (the Electriq EAP500HC) costs over £200.
Choose when and where you are going on holiday carefully, so you get away during the worst period. North of Scotland and the islands have a short, late grass season (late June, early July). Coastal areas likely to be best (although often there are fields just back from the coast, so it may depend on the wind direction!). For tree pollen, season is earlier for most (see above), and there are parts of Scotland (Orkney, Lewis, Caithness, Sutherland) with very few trees. For holidays abroad, see World pollen data.
Medicines
Antihistamines – oral, nasal or eye drops. Various, some people find one works better than another Sedating antihistamines eg Chlorphenamine should be avoided except at night.
Cromoglycate eye drops are available, they work in a different way from antihistamines so may give additional benefit. But need to be given 4 times daily, which is inconvenient.
Nasal steroids useful if used correctly. Fluticasone is licensed from age 4 – Betnesol nasal drops from age 2 (but systemic absorption an issue). Combination steroid/antihistamine spray available from age 12.
Leukotriene receptor antagonist licensed for hay fever in children with asthma.
Short courses of oral steroids might be justified for special occasions.
Immunotherapy available. Grazax is sublingual grass product; Pollinex Grass and rye is subcutaneous. age not important cf ability to hold in mouth for 2 minutes! Metanalysis by Dhami S et al of grass desensitization in children, using either subcutaneous or sublingual therapy, found overall standardized mean difference (SMD) of -0.53 (95% CI -0.63, -0.42) in symptoms scores (roughly equal numbers of SCIT and SLIT studies, roughly equivalent scores) [Allergy 2017]. Deaths reported in asthmatics with poor control.
Itulazax is NICE approved tree pollen daily sublingual (need to start 16 weeks ahead of season, so last week in November; £80 on NHS). Pollinex tree is subcutaneous.
Licensed but none approved by SMC (Grazax rejected in 2008 and not re-submitted, Pollinex and Itulazax never submitted) for Scotland. Combined grass and house dust mite products?
Omalizumab – monoclonal anti-IgE – single injection of 300 mg omalizumab two weeks before start of the pollen season achieves better overall control of symptoms and QoL [adults, China 2022]. Evidence of benefit in allergic rhinitis with difficult asthma [adults, 3 years worth of monthly treatment, Italy 2020].
Diagnosis is about probability – high probability is recurrent episodes of cough, wheeze, breathlessness, chest tightness plus documented wheeze, atopic history, documented variable PEF or FEV1. Isolated episodic cough is not sufficient. Episodes typically triggered by viral infections, cold air, exertion, laughter or emotion. Start treatment, “typically” 6 weeks inhaled corticosteroids (ICS). If good response to treatment, then diagnosis is confirmed.
If intermediate probability then spirometry with reversibility is preferred initial test for children old enough to do it (Grade D recommendation). If spirometry normal, then do challenge tests and/or Fractional exhaled nitric oxide (FeNO) measurement. For younger children, watchful waiting or trial of treatment [colour code suggests this is appropriate from age 1, but no advice given for under 1…].
FeNO has reasonable positive predictive value, but false positives in allergic rhinitis, rhinovirus and dietary nitrates, plus overlap in values between asthmatics and normal population (especially children).
Red flags –
Focal chest signs
Abnormal voice or cry
Failure to thrive
Vomiting
Wet/productive cough
Nasal polyps
Management
Self management education, written personalized plan. Assess control – consider using Asthma Control Test (ACT) questionnaire or similar.
Assess risk of future attacks. Co-morbid atopic conditions, younger age, obesity, and exposure to environmental tobacco smoke are markers of increased risk (some of these strongly socioeconomically linked, of course).
Ask specifically about medication use and assess prescriptions. Explore attitudes to medication as well as practical barriers to adherence.
Not for routine house dust mite avoidance measures. Avoid smoking and second hand smoke.
Weight loss (including dietary and exercise programmes) for overweight and obese. Breathing exercise programmes can be offered as an adjuvant to pharmacological treatment for adults.
Treatment
ICS are recommended preventer. An asthma attack in the previous 2 years, symptoms 3 days a week, or using reliever 3 days a week, or waking 1 night a week are indications. Give twice daily at least until good control established.
Start at dose appropriate for the severity of the disease. In mild to moderate asthma, no benefit in starting at high dose and weaning. In children, “reasonable” starting dose is Very Low (100mcg twice daily of Clenil or equivalent).
5yrs and over, if add-on is required then choice between inhaled long acting beta agonist (LABA) or leukotriene receptor antagonist (LTRA). Only then increase dose of ICS from very low (100mcg Clenil or equivalent twice daily) to low (200mcg twice daily).
For exercise induced symptoms, generally just a sign that inadequate control! But if otherwise well controlled then give inhaled short acting beta agonist immediately prior to exercise. Then choice between LRTA, LABA, cromoglicate or theophylline.
Acute Severe Asthma
Sats under 92%
PEF 33-50% of best or predicted
Can’t complete sentences in one breath, or too breathless to feed
HR >140 (under 5), >125 (over 5)
RR>40 (under 5), >30 (over 5)
Life threatening defined as:
PEF <33%
Exhaustion, poor resp effort [tautology?]
Hypotension
Cyanosis
Silent chest
Confusion
Treat –
Oxygen
MDI plus spacer if mild/moderate
If refractory to beta agonist, add ipratropium 250mcg mixed into beta agonist [same dose for everyone]
“Consider adding 150mg magnesium sulphate to each neb in first hour if symptoms started <6hrs and presenting with sats <92%” = 0.3ml of 50% MgSO4
Give oral steroids early, dose by age.
Second line treatment –
Consider single IV bolus of salbutamol (15mcg/kg over 10mins). For bolus dilute to 50mcg/ml with saline/glucose. For infusion, dilute to 200mcg/ml
Consider aminophylline for severe asthma unresponsive to maximal doses of bronchodilators and steroids. Loading dose slow injection over 20 mins! Then dilute to 1mg/ml with saline
Consider IV MgSO4 40mg/kg over 20 mins – dilute to 10% in saline or glucose.
Systematic review of IV Magnesium in children (2018) – pulmonary function improved, hospitalization and further treatment decreased. MAGNETIC trial of Magnesium nebs did not show a clinically significant improvement in mean asthma severity scores in children with acute severe asthma. But better Asthma Severity Score at 1 hour where saturations <92% at presentation and those with preceding symptoms lasting less than 6 hours [Lancet 2013]. 2022 Metanalysis found no benefit but varying protocols and populations.
Physiological is because Long chain FAs in breast milk compete with Glucuronyl transferase! Dehydration and poor feeding contribute (jaundice FOLLOWS, does not cause). But can also be seen in bottle fed babies.
Prolonged jaundice defined as 21/7 if well, term according to American Academy of Pediatrics. After that, investigation probably appropriate.
Unconjugated vs Conjugated bilirubin is important – do direct bilirubin. Conj bili >20 may indicate significant disease, esp if unconj not high. Low albumin suggests prenatal onset.
Unconjugated
Haemolysis (so liver function tests normal): eg rhesus disease (diagnosis: Direct Coombs Test Positive), ABO, irregular antibodies (Kell, Duffy; varying significance), hereditary sphero/elliptocytosis, G6PD deficiency, DIC. G6PD in baby can be precipitated by maternal drugs/infection. Enzyme assay false negative because of high retic count, so test mother for carrier status.
Crigler Najjar is unconjugated. Uridine Di Phos Glucuronyl transferase deficiency (Dubin Johson/Rotor only present >2 yr). Recessive form is severe, assoc with kernicterus; dominant can be treated with phenobarb.
Hypothyroidism
Galactosaemia – in the first week of life can be unconjugated but always features liver dysfunction cf Crigler Najjar so unlikely to be any confusion.
Conjugated
Suggests hepatitis. Note that Alk phos in normal neonates is often high in isolation. See BSPGHAN protocol.
Choledochal cyst: assoc with East Asians, PKD (Caroli’s disease). Cystic mass below liver. Can rupture and cause ascites, cause obstruction +/or cholangitis. Late carcinoma risk.
Can be due to mineral deficiency or toxicity. But can become habitual, in which case motives/consequences should be explored – attention? Escape? Sensory feedback?
Usually iron deficiency, but potentially calcium, zinc. Beware vitamin deficiencies esp C.
Lead exposure can come from toys sourced from outside EU. Houses in area built before 1950? Water companies generally screen for this, houses are occasionally notified of a hazard. But lead poisoning can also be a consequence of pica.
Complications are rare but potential for bezoar formation, gastrointestinal side effects. Toxocariasis if faeces is ingested.
Management
Ignore or avoid negative attention (eye contact, facial expression, speech)
Other oral stimulation eg. chew wristbands
Reward keeping hands in pockets?
Teach edible vs. Non-edible
Alternative communications methods
Provide similar smells, textures, colours to play with or eat
For suspected asthma, where child unable to do spirometry, then watchful waiting or trial of treatment for specified time period. Choice of treatment depends on severity and frequency of symptoms – “typically 6 weeks inhaled steroid”, “very low dose”.
Start regular preventer treatment or escalate treatment if you are getting frequent symptoms, viz:
three times a week or more, or
using your blue inhaler three times a week or more, or
if your asthma is waking you up once a week or more.
Start regular preventer if asthma attack in previous 2 years!
Same table for all ages now, and same steroid doses!
Step 1 – very low dose inhaled corticosteroid (ICS). OR leukotriene receptor antagonist (LRTA) if under 5.
Step 2 – Add LRTA if under 5, else inhaled long acting Beta agonist (LABA) if 5+.
Step 3 – If no response to LABA, stop and increase ICS dose. If some benefit from LABA continue and increase ICS dose, or consider trial of LTRA.
Step 4 – high dose therapies: increase ICS dose to medium, or add slow release theophylline. Refer for specialist care.
ICS doses
Very low dose is 50mcg 2 puffs twice daily of beclometasone. Low dose is double that, medium 200mcg 2 puffs twice daily.
QVAR and fluticasone are double the efficacy of beclometasone so doses are halved. Ciclesonide is somewhere in between.
An added sound heard when listening with a stethoscope, distinct from heart sounds or other clicks or snaps.
Can indicate a structural abnormality. But can be heard in normal hearts too, esp kids.
Still’s murmur
Or “innocent” murmur. Characteristic vibratory, low pitched, crescendo-decrescendo sound – “like an Aeolian harp” – loudest along left sternal border. Never louder than grade 3. Typically gets quieter when child sits or stands up (reduced venous return?) – you would not expect a murmur caused by a structural abnormality to change much.
Present at any age. Usually goes away by adolescence.
Venous hum
Another innocent one, a rumble heard in the upper chest, disappears when lying down, or when neck turned or neck veins occluded gently.
Pulmonary flow murmur
Pulmonary valve closest to anterior chest wall, which might explain why you sometimes hear this. Might be confused with pulmonary stenosis or subaortic membrane.
Baby strains and cries to pass stool but it comes out soft or not at all. Functional gastrointestinal disorder thought to occur in 0.9 – 5% of infants under 6 months (Rome IV criteria).
Due to poor co-ordination of pelvic floor muscles with increased intra-abdominal pressure generated during stooling. Seen in babies up to 9 months.
Studies have reported symptoms of discomfort around passing normal stool in up to 18% of babies, not all of these children will strictly meet the diagnostic criteria for dyschezia.
Differentiating from true constipation etc requires a clinical history and a normal clinical examination, with the key difference being that the stool is not hard in dyschezia.
No medication (or any form of rectal stimulation) required, can be expected to resolve spontaneously.