UK-PAS meeting (David Goldfarb from University of British Columbia – PID and micro.)
H5N1 first appeared in 1997 in China but no more cases until early 2000s.
2017 report lots of young children, high mortality (53%). Unrecognised cases never admitted?
New clade 2.3.4.4b in 2021 – crossing over to mammals in Americas. Last year some mild cases related to cows.
Death in Louisiana H5N1 2025 (not the clade in dairy farms), related to poultry (underlying health issues and over 65 years). H5N1 circulating in wild and farmed birds in Scotland, H5N5 back in wild birds.
2024 – 13yr old mild asthma, obesity (117kg), presented with conjunctivitis and fever. Then vomiting and dyspnoea, quickly transferred to PICU. LLL pneumonia. No risk factors.
Biofire resp panel used for PICU – includes pan influenza A antigens, so positive but H1/3 negative. Then did reflexive Xpert assay, which is quantitative. Relatively strong so referred to reference lab.
Genomics done within 4 days. Showed close to “cackling goose” strains. Also identified mutations associated with increased binding (not seen before in H5) so infectivity increased.
At same time Louisana case with same gene type and mutations.
Infection control tricky – new genes! Other studies have suggested incubation up to 13 days. Maintained airborne precautions until 2 negative samples (lower resp samples continued to be positive for 15 days, tracheal just 2 days…)
Note potential exposure to lab staff – discuss!
Ashraf Znait (PICU fellow) – intubated for hypoxia despite BipAP. Echo showed good function on intoropes. Started ECMO at 6 hours after intubation. Double cannulas (IJ and femoral) required to achieve sats of 80%. Dual lumen cannula. Required CRRT for fluid overload and anuria but high pressure with combination so switched to separate femoral dialysis catheter.
SIRS and haemodynamic instability persisted, decided against steroids (higher mortality in influenza cases 2019 – Recovery trial in UK currently?) so plasmapheresis.
D10 off inotropes. D15 before decannulated. D21 extubated.
Mode of acquisition never explained! No immunological problem found.
Ellie MacBain (PID fellow) – case series from 2012 found 75% increased risk of death with delayed oseltamivir treatment. IL6 and IFNgamma, resp sample viral load higher in fatal cases.
Oseltamivir resistance has been described in avian cases of this clade. WHO suggests higher doses (eg 150mg BD), combination therapy, or prolonged treatment.
This case had PCR positive serum with cycle threshold (CT) suggestive of true viraemia. Added amantadine, baloxavir, unable to procure IV zanamavir. From different classes of antiviral in any case.
Never positive bacterial cultures! On/off antibiotics throughout.
Ashley Roberts (Prof PID) – treatment doses used for oseltamivir prophylaxis, for 7-10 days.
Feno (if available) >35ppb diagnostic, age 5+. If not diagnostic, measure BDR with spirometry. Diagnose asthma if the FEV1 increase is 12% or more from baseline (or if the FEV1 increase is 10% or more of the predicted normal FEV1).
If spirometer not available, measure PEF twice daily for 2 weeks. Diagnose asthma if PEF variability (expressed as amplitude percentage mean – the difference between the highest and lowest PEFR readings on a given day, divided by the mean of those readings, averaged over period) is 20% or more.
Failing that, either positive skin prick testing to house dust mite or measure total IgE level plus blood eosinophil count. Raised total IgE plus Eos >0.5 considered diagnostic! [Because highlights underlying atopy cf viral wheeze?]
Under 5, prescribe steroids [not just salbutamol!] for 8-12 weeks and review. [No dosage guide for under 5s!?] Then do objective test when they reach 5! If no response, check technique, consider environmental triggers (mould, smoke etc), consider alternative diagnosis, refer.
If making asthma diagnosis, record basis for this in notes.
Management
Under 5, consider stopping ICS at 3-6 months or else within 12 months.
If helps but then symptoms recur, can try moderate ICS dose. After that, 8-12 week trial LTRA.
Uncontrolled = exacerbation requiring oral steroids, or use of SABA 3 days a week or more, or night waking once per week or more.
New section on diagnosis at time of acute presentation!
Refer to a specialist respiratory paediatrician any preschool child with an admission to hospital, or 2 or more emergency department admissions in a 12-month period.
Age 5-11, start low dose ICS. After that, assess ability to manage MART (maintenance and reliever therapy) regimen (none licensed under 12, so would be off label). Start low (Budesonide 100/3 MDI or 100/6 Turbohaler – see below for brands), 2 puffs/sucks per day in 1-2 divided doses), go to moderate (300-400mcg per day) if necessary. [No evidence for MDI, only for dry powder!]
Otherwise would be trial of LRTA, then add LABA, then increase ICS to moderate.
12+, start Anti-inflammatory reliever (AIR) therapy with prn combination ICS/LABA inhaler (only budesonide/formoterol licensed for this). This strategy had lowest rate of severe exacerbations (plus cheaper). WockAir is cheapest.
If highly symptomatic at presentation could start MART +/- oral steroids with view to stepping down.
If MART required and still symptomatic on moderate dose, check FENO and eosinophil count – refer if either high. Otherwise trial of either a LTRA or a long-acting muscarinic receptor antagonist (LAMA, eg tiotropium).
Beware neuropsychiatric side effects of LTRA/montelukast. Review annually.
Inhalers
Duoresp Spiromax 160/4.5 (powder, 12+ – on NHSL adult formulary) – For MART, 2 inhalations daily in 1-2 divided doses (up to 2 BD); PLUS 1 inhalation PRN for relief up to 8 in a day (up to 12 for a limited time but medical assessment recommended). Also comes in 320/9 but only for maintenance.
Symbicort 100/6 turbohaler (powder) 6+ for maintenance. 12+ for MART
Symbicort 200/6 (powder, 12+ – on NHSL adult formulary) MART as above. Else AIR – 1 puff PRN, up to 6-8 (up to 12 for limited time).
Symbicort 100/3 MDI 12+ MART – 4 puffs daily in 1-2 divided doses, up to 4 BD. 2 puffs PRN for relief up to 12-16 in a day (max 24)
Wockair 160/4.5 (powder) cheapest! (£19) MART 2 inhalations daily in 1-2 divided doses, up to 2 BD. 1 inhalation PRN up to 6-8 (max 12). Else AIR – as above
Fobumix 80/4.5 Easyhaler 6+ for maintenance, 12+ for MART.
Fobumix160/4.5 Easyhaler 12+ MART or AIR.
Non-pharmacological measures
House dust mite reduction measures not routinely recommended. Evidence on removal of pets from homes “paradoxical” – no benefit or tolerance if continued presence. If detectable cat antigens without cat, might be benefit to high efficiency vacuum cleaning or additional measures.
Air pollution linked to worse symptoms.
High sodium and low magnesium intake linked to asthma symptoms but poor/no evidence that intervention makes a difference. High intake of fresh fruit and vegetables is associated with less asthma and better pulmonary function but no interventional studies.
Weight loss interventions may help asthma symptoms in overweight/obese, and should be considered, but may require >10% loss for benefit.
Breathing exercises eg Papworth/Buteyko methods can lead to modest improvements in asthma symptoms and quality of life, and reduce bronchodilator requirement, in adults with asthma. Less evidence for effect on lung function or airway inflammation. Insufficient evidence in children.
Monitoring
Monitor asthma symptoms, plus check:
any admissions to hospital or attendance at an emergency department due to asthma.
time off work or school due to asthma
amount of reliever inhaler used, including a check of the prescription record
number of courses of oral corticosteroids
Asthma Control Questionnaire, the Asthma Control Test etc can be used.
FENO can be considered for monitoring in adults only. Peak flows not routinely indicated for monitoring.
Transition
Not much! Separate section on self management. Vaping/smoking. Factors that affect inhaler use eg school/social. Career plans.
A spectrum of disorders where the normal left-right arrangement of organs in the body is disturbed (“errors of lateralisation”).
Situs inversus is complete mirror image arrangement – there are no health consequences as a result (other than iatrogenic eg delayed diagnosis of appendicitis).
Many genetic causes. Primary cilial dyskinesia (Kartagener syndrome) is one.
Heart – IVC can be interrupted, requiring azygos veins to drain lower body vessels back to heart. Many variations of valves and connections seen. Congenital heart block often seen.
Seasonal lower respiratory tract infection of young children, typically caused by Respiratory syncytial virus (RSV) but can be others or mixed.
Classically wheezy cough, wheeze and/or crackles, reduced feeding and increased work of breathing.
Fever not usually high (“consider pneumonia if over 39”)
Diagnosis
Clinical. You would probably have to do 133 Chest x-rays before you found something that would change diagnosis – overuse of CXR associated with increased (and inappropriate) use of antibiotics.
Swabbing for virus identification can help with cohorting and avoidance of nosocomial infection, which can be a major problem.
Management
Ex-prems, chronic lung disease, neuromuscular disorders, haemodynamically significant congenital cardiac disease, immunodeficiency at higher risk, of course.
Admit if sats under 90% if 6/52+ (92% if underlying health problem or under 6/62) – and start oxygen if persistently low.
Admit if feeds less than 50-75% of usual volume, or severe respiratory distress, or reported/observed apnoeas.
NG or orogastric feeds if required – no preference but in theory obstructing nostrils could be unhelpful…
And UTI
Bacteriuria is not uncommonly seen with bronchiolitis, not always clear if this is true urine infection.
Prognosis
Initial coryza 1-3 days. Symptoms peak at 3-5 days. Cough resolves within 3 weeks in 90% but can persist for longer (but perhaps recurrent viruses?).
Prevention
RSV passive immunisation for high risk babies with paluvizimab (Synagis). Limited benefit but does appear to reduce incidence of severe bronchiolitis.
Vaccination in pregnancy effective – antibodies cross, but also prevents Mum getting it and passing it on!
JCVI recommended Nirsevimab be used first line in 2023 – single injection (half life 71 days). HARMONIE trial – 83% reduction in RSV hospitalisation, 75% reduction in “very severe” disease. Spain and US doing. Fight for global supply so not available…
2025 – programme for high risk babies extended to include all babies born <32/40 (regardless of whether mum received vaccine in pregnancy).
Initial studies did not show any relationship between moulds/damp and health, as there was major confounding with socioeconomic status, and because it is hard to quantify mould exposure (with many different mould species).
Then there is the effect of climate, and the built environment – heating, ventilation, insulation, materials etc.
More recently systemic reviews have made it clear there is a link particularly with development of asthma, particularly in older children, and where there is already a family history of atopy.
Coroner ruled death of 2yr old Awaab Ishak in 2020 from granulomatous tracheobronchitis was due to environmental mould exposure from poor housing.
Longitudinal studies have suggested that there may be protective effects but data is limited.
Similarly there is evidence that higher exposure to moulds leads to more asthma exacerbations.
There are genetic polymorphisms that affect ability to break down the fungal protein chitin, and these have been linked to urgent medical care visits, which suggests a non-immune mechanism may be important.
Dampness is linked to mould growth but also to house dust mite, microbial volatile compounds, mycotoxins and endotoxin.
The most studied mould species are Aspergillus, Penicillium, Alternaria and Cladosporium.
Limited evidence that interventions to reduce mould make any difference.
Le Chiffre in Casino Royale may use a custom metal inhaler, but the implication is clear – he is not as masculine as James Bond.
“Mikey from “The Goonies,” who is portrayed as vulnerable and nervous and is seen taking puffs from his inhaler whenever a situation is particularly scary. Stevie from “Malcolm in the Middle” who suffers from severe asthma can barely make it through a sentence without gasping for breath and wheezing uncontrollably.
“Though he is also proclaimed a genius, it is this perceived weakness that becomes his defining characteristic.
“The stereotype even translates to cartoons, with Carl Wheezer from “Jimmy Neutron: Boy Genius” and Millhouse from “The Simpsons” represented as weak and timid individuals who are used as comic relief whenever they are upset and need a puff from an inhaler to control their symptoms triggered by anxiety.” [American lung association blog]
In the film Hitch, the lovable accountant Alfred uses his inhaler when he is scared to take action. Until he is inspired to greater manliness, and he throws it away and mounts the steps to kiss his girl in passion, no longer shackled by his psychological, rather than medical, condition. [https://mbtimetraveler.com/tag/asthma-portrayal-in-television-and-movies/]
Even JK Rowling is guilty – see her TV show “The casual vacancy”.
Stephen King’s It has a hypochondriac asthmatic character Eddie Kaspbrak – although at least there is a genuinely terrifying scene where he has an asthma attack and his inhaler has run out – but even this has been triggered by bullying, enforcing the “nerd” stereotype.
Wheezy in Toy Story 2 is also a rather pathetic character.
Positive role models lacking. David Beckham and Harry Styles are some of the few.
Children with asthma, not surprisingly, are highly sceptical of such portrayals. Non asthmatic children obviously don’t appraise movie scenes for their meanings but they do judge the social context of the drama [https://pubmed.ncbi.nlm.nih.gov/22574393/]
Few if any other medical conditions seem to get the same treatment…
Obesity can mimic asthma, it affects respiratory symptoms and lung mechanics, but it can also overlap of course. Asthma is more often diagnosed in obese (misdiagnosed?). Maternal obesity (and gestational weight gain) in pregnancy. Each BMI increase of 1kg/m2 increases risk by 2-3%!
Obesity is one of the factors associated with fatal asthma attacks (but note socioeconomic confounding).
Weight reduction leads to improved lung function, health status, symptoms and morbidity in adults. Not yet proven in adolescents.
Slightly increased risk of acute asthma attacks in obese adults and school age children.
=allergic rhinoconjunctivitis due to seasonal triggers, typically grass and/or tree pollen, can also be weeds/moulds. First described by John Bostock in 1819, so a new disease!?
More likely if born in early months of year!?
So itchy, swollen, watery eyes, runny and/or blocked nose, sneezing. Often itchy throat and ears too. Cobble stone appearance can be seen at the back of throat.
Not dangerous, but can seriously affect quality of life: poor sleep, poor concentration (exams usually at worst time of year), embarrassment about snot. One study in England showed that children with hay fever requiring anti-histamines are significantly more likely (43%) not to achieve predicted exam grades, especially when using first generation sedating antihistamines such as Piriton (chlorphenamine) [Samantha Walker, JACI 2007: 120; 381-387].
Associated with other atopic conditions, such as food allergy and asthma. Moderate to severe hay fever also associated with worse, uncontrolled asthma. London study found hospital admissions for asthma 50% higher 3 days after high grass pollen levels (inconclusive for tree pollen). [Int J Biometeorol. 2017]Brussels study found similar, compounded by air pollution. Treatment of hay fever with intranasal steroids or class 2 antihistamines reduced admissions by up to 80%. [asthma res and pract2015]
Pollen is too large to trigger the lower airways directly, rather, pollen exposure in the upper airways trigger inflammation that travels down (probably over a period of weeks) to the lower airways. An exception is when pollen grains are fragmented, as seen in thunder storm asthma where one night in Melbourne, 2016, several thousand acute respiratory presentations came to ED (up over 600%), asthma admissions up over 900%, hospitals ran out of inhalers. 10 deaths implicated. [Australia, Clin Exp Allergy. 2018;48:1421‐1428]. Complex though, rain/moisture probably contribute to pollen grain rupture, and atmospherics bring surges of pollen down to ground level.
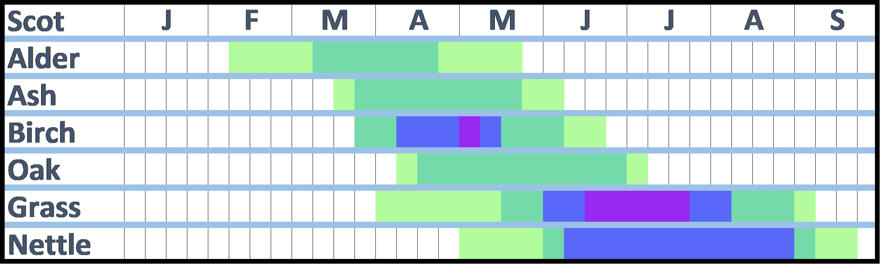
There are many different species of grass, but if allergic to one you tend to be allergic to all of them. Trees on the other hand vary, you tend to be allergic to specific groups of trees. In Europe the most important are birch (northern Europe) and olive (Southern Europe). Birch pollen cross reacts with alder, hazel, hornbeam, beech, oak, chestnut. Olive is related to ash and lilac, cross reacts to a degree with birch. Cedar and cypress are related, pine (spruce/fir etc) are different but latter pollens are heavier and thought not to be as relevant to symptoms. Weeds belong to various unrelated families.
Hazel trees can start producing pollen in January! Peak is Feb/March. Alder is next earliest (see chart below). Pine is quite late, similar to grass. Weeds such as nettle can continue producing pollen through September! Cypress blooms in winter!
Average start of grass season in Scotland is mid-May (dark green on chart below), high counts generally start 1st week of June (blue), peak (purple) is mid-June to mid-July. (Light green is earliest/latest appearance, low risk).
Average start of birch season in Scotland is last week in March, highest counts end April, early May.
It’s not just pollen count – the amount of allergen carried by the pollen (“pollen potency“) varies too. Correlates pretty closely but varies by time and place, 4-5 fold difference geographically (especially grass). France has the highest yearly average grass pollen potency, 7-fold higher than Portugal. Olive pollen from two locations 400km apart varied 4-fold in their allergen potency – in Portugal there are times when pollen from Spain probably more of a problem for triggering hay fever than pollen from “local” trees! [Health Impacts of Airborne Allergen Information Network (HIALINE project)]
Moulds seem more associated with asthma than hay fever.
Management
Watch the pollen count, and choose activities inside or outside accordingly. There are apps that can help with this. But note that the time of day is important too – for grass pollen, the risk is greatest in the first half of the morning and again from about 4pm in the afternoon, until late evening. But can persist into the early hours if temperatures remain high, this effect is particularly noticeable in the cities of the south of England. For tree pollen, the risk is usually during daylight hours only.
Closing windows, or at least not sitting near windows should help. Wash your hair more regularly. Don’t dry clothes outside. Pollen barrier balms available (evidence?). Big, wrap around sunglasses?
Air purifiers with a HEPA filter should help but doors and windows will need to be closed. Unfortunately the best ones tend to be big, expensive and noisy, and price does not mean good quality. Plus you have to remember to replace the filters. The cheapest Which? recommended one (the Electriq EAP500HC) costs over £200.
Choose when and where you are going on holiday carefully, so you get away during the worst period. North of Scotland and the islands have a short, late grass season (late June, early July). Coastal areas likely to be best (although often there are fields just back from the coast, so it may depend on the wind direction!). For tree pollen, season is earlier for most (see above), and there are parts of Scotland (Orkney, Lewis, Caithness, Sutherland) with very few trees. For holidays abroad, see World pollen data.
Medicines
Antihistamines – oral, nasal or eye drops. Various, some people find one works better than another Sedating antihistamines eg Chlorphenamine should be avoided except at night.
Cromoglycate eye drops are available, they work in a different way from antihistamines so may give additional benefit. But need to be given 4 times daily, which is inconvenient.
Nasal steroids useful if used correctly. Fluticasone is licensed from age 4 – Betnesol nasal drops from age 2 (but systemic absorption an issue). Combination steroid/antihistamine spray available from age 12.
Leukotriene receptor antagonist licensed for hay fever in children with asthma.
Short courses of oral steroids might be justified for special occasions.
Immunotherapy available. Grazax is sublingual grass product; Pollinex Grass and rye is subcutaneous. age not important cf ability to hold in mouth for 2 minutes! Metanalysis by Dhami S et al of grass desensitization in children, using either subcutaneous or sublingual therapy, found overall standardized mean difference (SMD) of -0.53 (95% CI -0.63, -0.42) in symptoms scores (roughly equal numbers of SCIT and SLIT studies, roughly equivalent scores) [Allergy 2017]. Deaths reported in asthmatics with poor control.
Itulazax is NICE approved tree pollen daily sublingual (need to start 16 weeks ahead of season, so last week in November; £80 on NHS). Pollinex tree is subcutaneous.
Licensed but none approved by SMC (Grazax rejected in 2008 and not re-submitted, Pollinex and Itulazax never submitted) for Scotland. Combined grass and house dust mite products?
Omalizumab – monoclonal anti-IgE – single injection of 300 mg omalizumab two weeks before start of the pollen season achieves better overall control of symptoms and QoL [adults, China 2022]. Evidence of benefit in allergic rhinitis with difficult asthma [adults, 3 years worth of monthly treatment, Italy 2020].