Wasting of biliary tree +/- gall bladder in early months of life (LANDING’s theory). Premature babies get it less (as wasting hasn’t progressed as much) but can still get it!
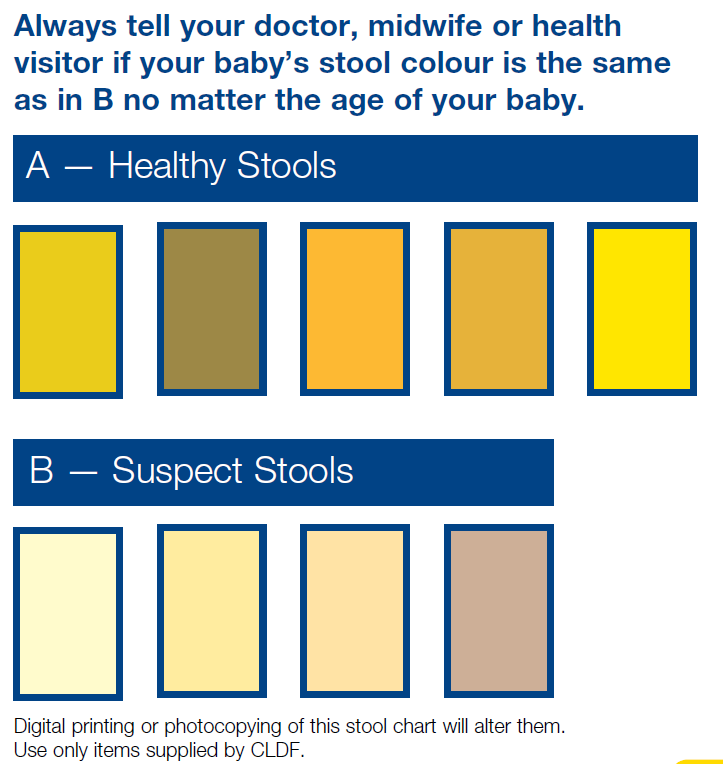
Presents with prolonged jaundice. Dark urine, pale (white!) stools distinguish it from common, benign breast feeding jaundice, but often missed. Parental reporting of stool/urine colour is unreliable! Stool colour chart available from Children’s Liver Disease Foundation.
Normally distal but 20% proximal.
Associated with SPLENIC MALFORMATION syndrome (poly or asplenia, situs inversus, malrotation, absent IVC).
Lanarkshire incidence 1.26 per 10 000, significantly higher than rest of Scotland! NO evidence of genetic factors. Pigweed in pregnant ewes in Australia – “biliatresone” toxin. Industrial waste…?
Investigations
Colour of stool!
Fasting (4hrs) USS essential, but sensitivity is operator dependent
Treat by Kasai Porto-enterostomy before 6 weeks ideally (16% normal LFTs, 18% portal hypertension, 94% survival @5yr +/- transplant), else liver transplant.
1yr phenobarb, urso, Vit K. Long term Dalivit.
Consider varicella vaccination if likely for transplant!
Prognosis
Prognosis related to clearing of jaundice, established cirrhosis/fibrosis, cholangitis, biliary stricture, portal hypertension (degree of – most have).
60% clear jaundice, up to 60% require transplant in first 2yrs. Of the rest, half need transplant in childhood, leaving just 20% getting to transition with native liver.Most mortality due to transplant complications.
New Japanese data suggests length of jaundice more important than age (traditionally 45-60 days low risk for liver failure)
Outcomes from Kasai operation are better in centres doing more than 5/yr, so only 3 supra-regional centres in England. But outcomes in Scotland seem to have got worse, even though overall better! Up to surgeon whether feasible or not for an individual patient.
Increased sepsis due to gut organisms from Roux-en-Y loop.
Cholangitis – features can be seen on USS. Characteristically unwell, febrile with rise in bilirubin and LFTs (but not always). Rx Tazocin. Some require antibiotic prophylaxis.
Portal hypertension can develop early or late. May present with variceal bleeding, low platelets, splenomegaly. Managed by banding of varices, TIPS shunt, transplant.
Strictures present with biliary stasis, itch, pain, coagulopathy.
[Rachel Tayler]