The UK still currently follows the European Food Information For Consumers Regulation (FIR) that took effect from December 2014.
This applies to unpackaged food eg restaurants, takeaway’s deli’s, bakeries etc. It now also applies to food prepacked for direct sale (PPDS) such as a sandwich made on the premises of a cafe but wrapped (Natasha’s law).
Allergy advice boxes are no longer permitted, although “may contain” advisory labels are. The allergen should be emphasised in the ingredients panel through typeset eg font, style, colour. The specific type of cereal or nut must also be stated.
The 14 allergens that must be highlighted under UK/European law are: cereals containing gluten (wheat, barley, rye etc), crustaceans (eg shrimp, prawn), molluscs (eg mussel, oyster), eggs, fish, peanuts, nuts, soybeans, milk, celery, mustard, sesame, lupin and sulphur dioxide at levels above 10mg/kg, or 10 mg/litre, expressed as SO2. Lupin and Molluscs added later.
There are some exceptions, where the food is so highly processed that they are no longer capable of triggering an adverse reaction eg fish gelatine in beer/wine, soya in vegetable oil.
If your allergy is not one of those listed, eg lentil, there is no legal duty for the manufacturer to highlight the presence of that ingredient, or for the restaurant to provide a full list of ingredients. So you need to read the full list of ingredients carefully, and plead with the restaurant for details relevant to your allergy. In the past, some manufacturers highlighted allergens in a separate box, but this is no longer permitted.
The rules list nuts as:
almond,
hazelnut,
walnut,
cashew nut,
pecan nut,
Brazil nut,
pistachio nut,
macadamia nut or Queensland nut
and products made from these nuts.
Other types of nuts, and other foods which are not nuts (even though they are called nuts i.e. chestnuts, pine nuts and coconut), are not named in the rules, even though they are known to cause allergy in some people.
Note that by law, “cereals containing gluten” includes oats! Spelt and Kamut should be declared as containing wheat. Oats contain avenin, rather than gliadin, but related. Products containing oats that have not been contaminated by wheat can be declared “gluten free” by law, so effectively the law considers oats as both containing but not containing gluten…
(food.gov technical guidance on new labelling law)
There is no legal duty to highlight changes in recipes on packaging. The same product with the same packaging can sometimes have different ingredients, depending on where it is produced.
The Food Standards Agency (FSA) has ordered councils to encourage restaurant owners to check their ingredients.
Note that non-EU countries will have their own rules eg US has only 10 ingredients that must be highlighted (not molluscs, mustard, celery, or lupin).
A good proportion of healthy children will have palpable lymph nodes in the neck. Mostly these will be under 1cm in diameter. Acute enlargement as part of an upper respiratory tract infection is usually accompanied by tenderness, and affected nodes will reduce in size over 4-6 weeks.
Guidance from NICE and the Scottish Government provide criteria when children with lymphadenopathy should be urgently referred for suspected cancer.
These criteria include the following:
lymph nodes are non-tender and firm/hard
lymph nodes are greater than 2 cm in size
lymph nodes are progressively enlarging
other features of general ill-health, fever or weight loss
the axillary nodes are involved (in the absence of local infection or dermatitis)
the supraclavicular nodes are involved.
But caveat is “Always refer any patient with Repeat presentations (3 or more times) of any physical symptoms which do not appear to be resolving or following a normal pattern, taking into account parental and patient concern”.
No need to do bloods in the absence of any of these criteria. Not that cancer is the only concern – differential includes developmental lesions (branchial cysts etc), TB, Cat-scratch disease, non-tuberculous mycobacterial infection (esp in neck). These are always more than 2cm and there may also be systemic features and/or overlying skin discolouration too.
Malignancies often present in the head/neck region. Hodgkins lymphoma usually affects teenagers, Non-hodgkins tends to affect school age children, neuroblastoma tends to affect pre-school children. B-symptoms (recurrent fever, weight loss, night sweats, pruritus, lethargy) are only seen in a minority but does suggest more advanced disease, of course. Airway or voice changes, swallowing difficulty, Horner’s syndrome, superior vena cava syndrome may all be seen due to mass effect. Most neuroblastomas have an abdominal mass. Nasopharyngeal carcinomas are seen so look in the nose/throat.
Failure to dilate, failure to contract (usually exogenous anticholinergic, such as Hyoscine patch gone AWOL)?
Is eye lid sagging? Is skin dry? Reflexes?
Hornersis small pupil with ptosis and dry skin – apical tumour (Pancoast) or lesion in brainstem/neck.
Dilated pupil can be part of third nerve palsy but you would usually also see ptosis and loss of adduction. Adie pupil is sudden onset mydriasis (dilated) with loss of reflexes (usually just ankle jerks) on the same side, can spread to other side. Usually post viral. Can be excessive sweating. Loss of reflexes can be permanent.
Physiological anisocoria = size difference does not vary according to light/dark.
Immunoglobulin A deficiency is the most common primary immunodeficiency.
1 in 700 healthy Western blood donors, but much rarer in some ethnic groups. FH only in a quarter.
Defined as a serum IgA concentration of < 0.06g/L in patients over 4 years of age, with normal levels of IgG and IgM, which is not secondary to other causes e.g. myeloma.
IgA subclass (IgA1 and IgA2) deficiencies described. IgA deficiency may be found in ataxia-telangiectasia, and IgG subclass deficiencies, drugs (phenytoin, sulfasalazine), chromosomal abnormalities (esp chromosome 18), coeliac disease.
Sometimes seen in families as recessive trait, else dominant with variable penetrance.
Issues:
Infection – Most individuals with IgA deficiency are clinically asymptomatic. Otherwise, higher than usual frequency of respiratory (incl sinus) infections, and GI infections esp giardiasis. Recurrent infections more often seen when accompanying IgG subclass deficiency (so consider IVIG, although contains small amount IgA, so might produce antibodies).
Associated conditions – Long term follow up has found higher rate of gut and lymphoid malignancies. Increased frequency of coeliac disease, autoimmune disorders and allergy/atopy.
Blood transfusion – IgA deficient patients can develop anti-IgA antibodies to blood products (20-40%). But these antibodies also seen not uncommonly in normal population and do not help predict transfusion reactions, so testing controversial. Severe reactions are v rare (1 in >20,000 transfusions).
Enhanced surveillance for transfusion reactions recommended, and pre-medication with hydrocortisone/chlorphenamine should be considered.
If a patient has previously had a reaction, then plasma reduced products or IgA def donor products (best) recommended. However, danger of delaying transfusion must be weighed against potential risk.
Transfusion labs should be informed of patients with the diagnosis.
Pathogenesis of IgA deficiency is presumably abnormalities in Ig class switching. T-cell function normal in most. Possibly part of CVID spectrum?
Binge Eating Disorder (without the compensatory behaviours of bulimia eg vomiting, exercise)
Selective/Restrictive Eating
DSM-IV Criteria for Anorexia Nervosa
Body weight at or below 85% of that expected
Fear of gaining weight or becoming fat, even though underweight
Disturbed perception of body weight or shape
Amenorrhea, at least 3 consecutive cycles
Disturbance in way one’s body shape is experienced (?)
ICD-10 adds a couple of things:
BMI < 15
Weight loss caused by food avoidance, self induced vomiting, purging, excessive exercise (not in DSM)
loss of libido in men
Pubertal delay if early onset
For children, these strict criteria can overlook significant disordered eating – wide variation in weight and height gain through puberty; menses not present else irregular. Levels of cognitive development obviously vary. Abnormal food behaviours eg slow eating, hiding may have been present from a young age. One type of eating disorder can change into another.
Interest in healthy eating and exercise may initially give impression that child is well. Dieting is miserable for most people, but for some it appears to relieve anxiety, which can lead to a vicious cycle. Sometimes it is specific foods that are feared.
BMI <2nd centile prob more useful for kids. GOSH Criteria (Nicoles, Chater & Lask 2000) talks about determined wt loss, abnormal cognitions about weight/shape but also morbid preoccupation. Similarly, Bulimia Nervosa defined as Recurrent binges and purges, Sense of lack of control, Morbid preoccupation with weight or shape. Purging is any behaviour to prevent weight gain including self induced vomiting, fasting, dieting, excessive exercise, misuse of medicines such as diuretics or laxatives.
Questions:
What did you eat yesterday? Are there foods you don’t eat any more?
Are you more interested in food and cooking?
Are you trying to cut back?
Does it ever feel like your eating gets out of control?
What happens if you can’t exercise?
Have you been making yourself sick? Do you drink water to prevent hunger?
What do you see when you look in the mirror? (Body dysmorphia = perception of shape, size that is unrelated to reality). Is there a weight you would like to be? What sort of things do you look at online?
Explore mood and risk of self harm. Anhedonia (inability to enjoy anything)common. Ask direct questions about abuse or neglect (explain this is routine).
Early intervention associated with better outcomes. Poor outcome in anorexia if patient does not receive effective treatment in first 3 years.
Principles –
Give diagnosis – may not be appreciated. Anosognosia = inability to see weight loss or failing health (and therefore others with that viewpoint are irrational or unkind)
Strengthening family relationships away from food (in many families tends to be around meals, snacks, eating out, and many conversations around favourite foods etc)
Conceptualising the eating problem as being separate from the young person. Eating problem as “bullying voice”. Avoid discussions of weight or body image (“you look healthier” can be misinterpreted as “you look fat” by eating problem).
Not a choice, not rational. Alexithymia (inability to express feelings) common. Genetic heritability accounts for approximately 50–80% of the risk of developing an eating disorder, often pre-existing tendencies towards anxiety, inflexibility, difficulties with emotional regulation, enhanced sensitivity towards punishment. [Proposed mechanism here]
Families are not to blame!
Food is medicine. Enforcing regular, balanced meals and snacks (3 of each daily) as a family improves mood, behaviour as well as physical symptoms. Terrifying at first, of course. Metabolism often ramps up once refeeding begins, so a huge increase in intake is often required to achieve restoration of healthy weight (and catch up growth) in anorexia. For bulimia, regular pattern of eating more important.
Don’t allow meal choices or negotiation, discourage involvement in or observation of food preparation, which reinforces disordered thinking. Reduces anxiety when not required to make “difficult” choices about problem foods.
Avoid regular weighing and other forms of body checking
Full recovery is possible, especially when detected early eg months rather than years.
Can be helpful to offer option not to be told weight. Beware concealing weights on body, water loading before weighing day. Praise honesty, highlight confidentiality, agree sharing of information with parents.
Parents can become used to “new normal” of disordered eating, and might not appreciate risks. Alternatively, young person might feel threatened by alliance between doctor and parents.
Target weight is tricky – what is required for normal bodily function? What was growth/puberty trajectory before eating restricted? So healthy thoughts about food, normal periods (often 9 months or more), return of premorbid personality etc. Fluctuating weight gain may be due to metabolism, fluid shifts, concealed weights or water loading, concealed purging (silent exercise eg crunches in bed).
Where food refusal is an issue, energy dense food is required – increase fat content, avoid water or diet drinks, leave fruit/veg till after other foods eaten. Smoothies or milkshakes often better tolerated. Bloating and nausea with refeeding common initially but should improve.
Family based treatment is recommended by NICE as first line. Emphasises that parents initially take back responsibility for feeding, then gradually handing it back to the young person. Minimisation of blame. If ineffective then CBT.
Psychotropic medication not recommended – metanalysis found no benefit from antidepressants in anorexia.
No evidence based guidelines for re-introduction of nutrition/energy in adolescents!
For the majority of patients, 40kcal/kg/day (1200kcal/day) appears to be safe – don’t start a meal plan with less calorific content than they were receiving prior to admission, although difficult when history of the amount taken is unclear.
The meal plan should comply with normal macronutrient guidelines (10-15% protein, 30-35% fat, 50-60% carbohydrates).
Increase the meal plan by 200kcal/day until 2000kcal/day is achieved.
Fluid 50ml/kg/d for 15yr+, 55ml/kg/d 11-14yr (Shaw et al). GOSH use standard paediatric fluid requirement calculations.
Promote weight gain 0.5kg/week (NICE 2004, Junior Marsipan 2012). Ignores malnutrition, of course. Percentage weight for height used, but easiest to divide BMI by median BMI for age/sex – 85% is underweight, 90% is satisfactory.
Check electrolytes, calcium, phosphate, magnesium, liver function, vit D on admission. QTc must be calculated MANUALLY (to find end of T, draw tangent through steepest part of curve).
All patients should be prescribed prophylactic dose of Vitamin D at a dose of 800IU/day whilst waiting for Vitamin D levels to be reported.
Prophylactic phosphate should not be routinely prescribed, however it should be considered where:
There has been a previous history of re-feeding syndrome.
Multiple risk factors
Consider Thiamine where starvation has been very prolonged (e.g. greater than one year at very low weight and poor intake) or there is a concern about vitamin deficiency.
A low phosphate (<1.1 mmol/L) before initiating feeds is unusual (see below) and should be corrected as soon as is possible on the day of admission:
Low phosphates should be discussed with the responsible consultant.
Give two sandoz-phosphate tablets and commence TDS regular phosphate regime.
Recheck U&E in 12 hours and monitor clinically (see below).
Do not make any increases on the feeding regime until phosphate has been corrected.
If phosphate is still low at 12 hours then consider repeated double dose, or IV correction. This is unusual.
Other causes of low phosphate should be excluded – in particular Vitamin D deficiency and hypoparathyroidism: check PTH and Vitamin D with next set of bloods (if hasn’t already been checked). These bloods should not hold up commencing of feeding once phosphate is normalised.
If phosphate is significantly low (<0.5) consider IV replacement – this will generally mean transfer to a medical ward.
Phosphates that are potentially dangerously low (<0.3) should be managed on a medical ward/PICU and discussions should occur with the consultant and CSPs about transfer before commencing feeding.
Refeeding syndrome
Biochemical abnormalities AND cardiovascular and neurological findings. Onset is in first 48 hours, up to first five days of initiating feeding (cases up to 18 days later described -consider at risk for up to 20 days). Cardiac arrest has occurred.
Early finding is drop in phosphate (increased requirement as body switches back to carbohydrate metabolism, plus chronic phosphate depletion due to starvation). Potassium, Mg also fall.
All patients considered at risk of re-feeding syndrome should be monitored for clinical signs of the re-feeding syndrome:
Resting tachycardia (differential for this includes anxiety).
Oedema or swelling, especially in the legs.
Confusion or altered conscious state (always check glucose in this case).
Patients should have:
Daily inspection for any signs of oedema (in particular peripheral oedema) for first five days.
Three times/day resting pulse and lying and standing blood pressure for first five days.
Monitor for biochemical/blood parameters of the re-feeding syndrome:
Daily urea, creatinine, sodium, potassium, phosphate, magnesium daily for five days. The drop in phosphate seen when re-feeding will normally occur within 48-72 hours.
Paracetamol prolongs clearance of malaria, and time to total scabbing in chickenpox. So only give for symptomatic benefit, not as routine!
Cochrane did not find any evidence that drugs prevent febrile convulsions, but not much data. Not recommended. Tepid sponging probably does work, but is inferior to drugs.
Ibuprofen probably works a bit quicker, and lasts longer. [Arch Peds Adol Metanalysis, 2004. PMID 15184213]
Alternating paracetamol and ibuprofen was superior in an Israeli study and in a US study.[Arch ped adol 2006 PMID 16461878, Clin peds 2008 PMID 18539869]
Combined? PITCH found combination was more effective than either alone (reducing time with fever over a 24 hour period by 2.5 hours or more) although it did not work faster than ibuprofen alone. No specific benefit was found for symptoms although it was underpowered for subjective comfort. [BMJ 2008 PMID 18765450] A linked cost benefit analysis suggested financial benefits to society for using the combination. On the other hand, use of the combination was associated with significant rates of medication errors and it could be argued that this risk outweighs the potential benefits.
Ibuprofen used as an antipyretic in febrile children with a past medical history of asthma is as least as safe as paracetamol and not likely to exacerbate asthma. [Lesko, Peds 2002]
NICE says:
Antipyretic agents (drugs that reduce fever) do not prevent febrile convulsions and should not be used specifically for this purpose.
When using paracetamol or ibuprofen in children with fever;
continue only as long as the child appears distressed
consider changing to the other agent if the child’s distress is not alleviated
do not give both agents simultaneously
only consider alternating these agents if the distress persists or if it recurs before the next dose is due.
[NICE feverish illness update May 2013 – new CG code: 160]
More than 10 years ago, shown to be effective in children – 2014 Andrew Clark Lancet STOP II study – 39 children 7-16yrs, peanut flour orally. 2 weekly up dosing, starting with 2 mg, increasing to 800 mg of peanut protein (5 peanuts) then maintained for total of 26 weeks. Tolerance then assessed with challenge.
91% achieved final daily dose (although only 62% actually had negative challenge, which was to 1400mg, nearly double – and previous evidence has suggested that most people at this level can tolerate substantially more with only mild symptoms).
Side effects mainly oral itching (6% of doses), nausea, vomiting. 1 patient needed IM adrenaline (twice) for wheeze. Even minor reactions are annoying especially GI, or if daily! And not always predictable. Tend to get less over time, of course. Paul Turner feels adverse event reporting “massaged” somewhat (no international consensus on reporting) – the word anaphylaxis not used except to thank the Anaphylaxis campaign, yet 22% of patients had wheeze at some point, even though reported rate of wheeze is 0.4% of doses. Still, anaphylaxis in hospital when potential reaction expected not the same as unexpected reaction in community.
Peanut IgE significantly reduced but not SPT! So works as long as you keep taking your daily dose, definitely side effects incl anaphylaxis, but not a cure.
No data yet on rates of reactions after treatment. But using anxiety model, OIT helps with “perception of severity” (as lots of minor reactions), “perceived ability to cope” (as managed already) and “rescue factors” (as more used to carry medicines). Note how experience of using AAI seen as positive (and kids often laugh at anticlimax of it!). 1/3 of benefit of OIT seen after initial confirmation challenge, particularly where anaphylaxis occurred (and in patients as well as parents)! [Sarah Burrell, ADC 2021]
Roughly 10-20% don’t desensitize at all. A further 10-20% don’t achieve full dose. And another 10-20% fail to achieve pass full dose challenge. Benefit likely to be highest for those most at risk of anaphylaxis, yet tendency will be to cherry pick lowest risk cases…
AR101 Oral Immunotherapy trial (PALISADE) – multiple authors including Jonathan Hourihane and George du Toit. US/Europe, N=496 aged 4-17yrs. Dose escalation then 24/52 maintenance (so about 12 months total) with peanut derived product, 67% passed 600mg peanut protein challenge (equivalent to 5-6 peanuts). [Some adult patients included initially but unsuccessful in all of them!]
Frequent mild/moderate events, but also in placebo group! 4.3% had severe events cf 0.8% of placebo group. About 10% withdrew due to adverse events , mostly GI- interestingly another 10% were lost due to parents withdrawing consent, I wonder what their reasons were.
Michael Perkins NEJM editorial – possible risk of eosinophilic oesophagitis? Only 1 case confirmed.
Second trial, just in Europe (ARTEMIS), n=227, up dosing every 2 weeks, just 12 weeks maintenance (300mg), so about 9 months treatment total. 58% tolerated 1000mg peanut (about 8-10 peanuts). Again, lots of mild/moderate adverse events but in the controls too! 1% rate of severe in treatment group (1 patient). 10% withdrew due to adverse effects. No eosinophilic oesophagitis reported. “Clinically important” improvements seen at the time of final food challenge in QOL scores related to “Allergen avoidance and diet restrictions” and “Risk of accidental exposure”, and in FAIM domains relating to perceived likelihood and chance of dying (both self and parent/carer reported) in the future.
Follow up study of self selected group of those who successfully completed 1yr PALISADE programme, who then opted to continue treatment for total of 18 vs 24 months – 48% of former still able to tolerate 2000mg, cf 80.8% of latter. Less adverse events over time of treatment, improved quality of life scores (“clinically meaningful”). Still peanut SPT positive (IgE a bit less for the 24 month group)! There were more accidental peanut exposures in this study than in the original trial, suggesting less vigilance, but the severity of these reactions and need for adrenaline was low, which might confirm an immunomodulatory effect.
Another follow up study (ARC004, Vickery) looked at daily vs non-daily dosing (6 months twice weekly 300mg) after PALISADE. Non-daily dosers had 40% more adverse events, although 80% mild-moderate. Daily dosers had best evidence of desensitization – more than 70% passed 1000mg challenge with NO symptoms (better than PALISADE), and 69% of the cohort (“3A”) who did 2yrs plus could do 2000mg with no symptoms. Evidence of “ongoing immunomodulation” with extended dosing – IgE reduced, SPT did not.
Does not discuss whether non-daily dosing might be appropriate for subgroup who have best immune response to treatment.
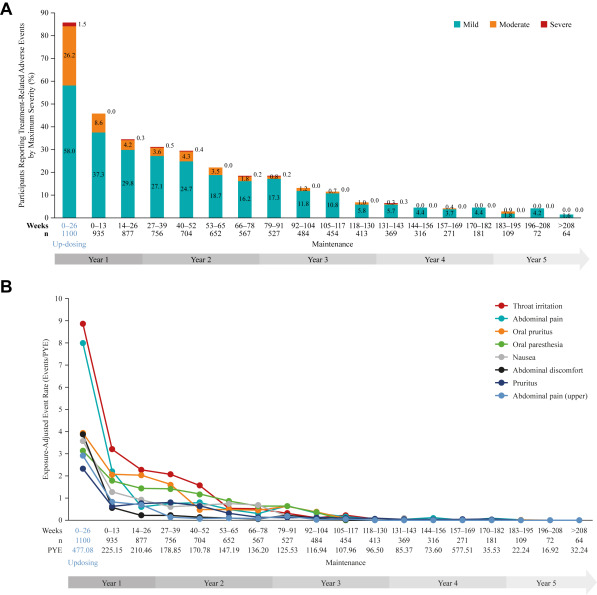
ARC0008 study still to report (closed 2023), but provisional data reported show the trend towards decreased adverse events (AEs) at years 1 and 2 is maintained up to 5 years, with 94% of patients experiencing mild or moderate AEs and only 13% discontinuing PTAH use because of AEs overall.
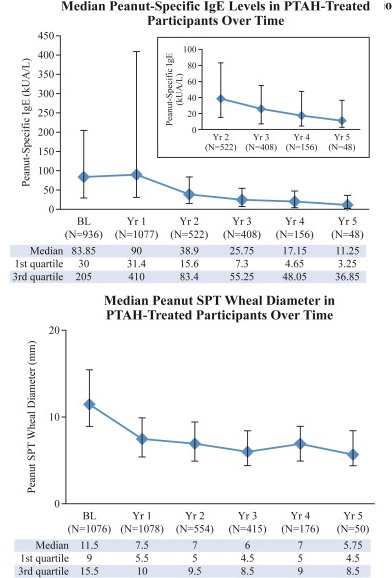
Gastrointestinal symptoms were the most commonly reported treatment-related AEs. A downward trend in systemic allergic reactions was also reported. PTAH treatment resulted in reduced levels of peanut-specific IgE after the first year and increased levels of peanut-specific IgG4, with a lowered peanut-specific IgE:IgG4 ratio. A reduction in median peanut skin prick test wheal diameter was observed (11.50 mm at baseline vs 5.75 mm at year 5). Unpublished draft is available here.
Severe and uncontrolled asthma was an exclusion criterium, obviously. Similarly chronic/recurrent abdominal pain.
AR101 (Palforzia) has now received NICE approval for use in NHS England, which has set targets for patient numbers. In Scotland, SMC did not find sufficient evidence of economic benefit, which fits with ICER report (US economic review) 2019 which showed that peanut immunotherapy led to more systemic reactions and more adrenaline use with no cost benefit. But hard to quantify benefit of reduced anxiety and increased quality of life. Natasha trial currently looking at immunotherapy using commercial peanut flour across several UK sites.
Various forums about immunotherapy. One young person’s blog is Ask About My Peanut Allergy (stopped regular peanut!!! But doing well).
Future may be to combine different routes eg sublingual/patch.
Study of accidental scalds/burns in 1215 children, looking predominantly at issues of prevention:
72% were <5 years, peak prevalence in 1-year-olds.
Commonest scald agent <5 years was a cup/mug of hot beverage (someone else’s, obviously).
Scalds affected the front of the body in almost all (96%): predominantly to the face, arms and upper trunk in <5-year-olds, compatible with pulling on an adult’s arm. Older children had scalds to the lower trunk, legs and hands.
Contact burns (<5 years) were mostly from touching hot items in the home, esp hair straighteners, irons and oven hobs.
Many contact burns in older children happen outdoors.
67% of all contact burns affected the hands.
Arch Dis Child doi:10.1136/archdischild-2013-304991 A M Kemp, S Jones, Z Lawson, S A Maguire
Used for assessing hypermobility, in other words lax joints (“double jointed”).
1 for each side of passive dorsiflexion of 5th MCP to 90deg, opposition of thumb to volar aspect forearm, hyperextension of elbow/knee, and placing of hands flat on floor with straight knees.
4+ needed for hypermobility syndrome (for adults), other major criterion is arthralgia for 3+ months in 4+ joints. Minor criteria include:
Other features of hypermobility syndrome in childhood include late walking, poor ball catching and handwriting, tiring easily.
Adults often get autonomic dysfunction eg orthostatic intolerance, functional bowel problems. Chronic pain syndrome and downward spiral in mobility often seen.
Ehlers Danlos syndrome has many proposed subtypes, some of which are pure hypermobility, but in others hypermobility may not be very obvious at all (just fingers!?). Some types have severe cardiac complications.
Design of hospital wards and symbolic practices try to maintain continuities with life at home. For young people though, the “childhood” presented may not resonate with their own sense of self and identity. “Sick child” contradicts modern cultural values of children being “priceless”, the value placed on futurity. Great Ormond St originally treated only children between 2 and 10yr – beyond that was considered not to need any different treatment!
Childhood now up to 18, according to UNCRC. The existing watershed of 11yrs and entry to high school is not recognized in hospitals. Children’s wards not seen as being scary, rather full of familiarity. Nor a place for respite from work, duties – rules exist about when TVs can be used etc that mirror school routines. The fact that family members continue to provide care is another continuity.
For young people however, things are rather different. They dislike the baby-ish aspects of ward decor or age-inappropriate toys/facilities.
The institutionalization of childhood has led to young people spending less time in adult society, or with their family, and more in age-based institutions – even when at home, they can spend a large amount of time communicating with their peers, away from the gaze of their parents. This does not happen in hospital. It is difficult for friends to visit, and mobile phone use is restricted. And the strangeness that does exist in hospital can create a sense of social isolation – this being an environment your friends wouldn’t want to be in.
For YP, being in hospital curtails their (new) independence, and subjects them to intense parenting that they may no longer be familiar with. Little room for possessions, for personalization. Loss of privacy esp bathrooms a concern.