Meaning typhoid and paratyphoid infection.
Typhus means smoke, refers to clouded consciousness characteristic of typhus and typhoid.
S. paratyphi treated the same but milder.
Pretty non-specific presentations – although called enteric, not striking vomiting/diarrhoea, in fact can be constipated…
Intracellular organism… Gall bladder and Peyer’s patches become focuses of infection (including chronic infection). Incubation period 10-14 days (up to 30!).
3 sets of blood cultures and stool cultures!
Typhoid Mary was Irish-American cook who was an asymptomatic carrier and caused at least 80 cases of typhoid in New York – her signature dish was peach ice cream… Asymptomatic carriage was not known about until her case investigated, she was told not to continue working as a cook but was not offered compensation. She was quarantined for 30 years of her life, the last 23 essentially in solitary confinement on an island off New York… Pretty harsh.
Clinical
Abdominal tenderness common. Rose spots (maculopapular, contain organisms!) hard to see in non-Caucasian. Less than 1 in 4 have them. Bradycardia with fever in first week. Hepatosplenomegaly in up to 50%. Nothing specific otherwise, but see complications below…
Complications
- GI bleeding and perforation
- Cholecystitis
- Pancreatitis
- Myocarditis/pericarditis
- Osteomyelitis
- Pneumonitis
Diagnosis
Culture from blood or bone marrow is gold standard. Stool culture could potentially pick up aysmptomatic carrier with another febrile illness… Low sensitivity anyway, esp first week.
Serological tests poor sensitivity/specificity (cross react with other Salmonella types).
Treatment
Always treat, even if well and only from stool (cf other salmonella types).
IV ceftriaxone if sepsis/shock, GI bleeding, intestinal perforation, encephalopathy, metastatic infection, total 10-14 days. Else azithromycin (loading dose 1g, 500mg daily 7 days; children 20mg/kg). [UK-PAS] For areas of high resistance and sepsis, Meropenem plus azithro [CDC Yellow Book].
Normal for fever to take 3-5 days to settle. After that, look for persistent locus and consider additional antibiotic. Fever can persist for 10 days with cefalosporins (low intracellular penetrance).
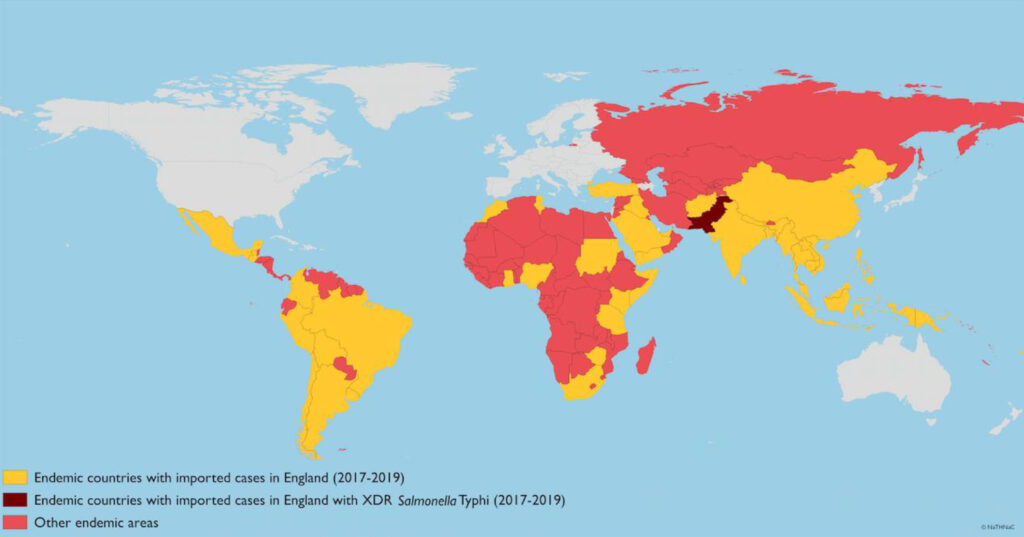
Drug resistance is a big problem. Fluoroquinolone resistance in most of Asia and sub-Saharan Africa. Oral third generation cephalosporins are also effective although inferior in RCTs.
Where nalidixic acid resistant, in vitro susceptibility to quinolones definitely reduced – use of maximum permitted doses and extending treatment course to 10-14 days will result in cure in >90% of cases — although the clinical response is slower.
Lots of data on quinolone use in children, but theoretical risks so Azithromycin preferred although response possibly slower.
[BIA guideline for England 2022]