The Uvea is the term for the whole eye (uvea=peeled grape). Whereas conjunctivitis looks like a red eye, it’s only really the surface that is inflamed. With uveitis, all the different tissues of the eye are inflamed. Acutely, might not look that different to conjunctivitis but painful, whereas latter usually just itchy. Anterior chamber starts to fill up with inflammatory cells so vision starts to deteriorate. An irregular pupil due to synechiae can eventually be seen, with hypopyon. Cataracts and scarring can follow.
Chronic on the other hand can be subclinical but potential for visual loss so screening important in associated conditions.
Usually idiopathic, otherwise:
Juvenile idiopathic arthritis – about 10% of patients with non-oligoarthritis, and 30% of ANA positive oligo so pretty common
HLA-B27 – with or without other B27 conditions such as Ankylosing spondylitis
Block DNA synthesis by bacteria (uniquely among antibiotics).
Good against gram negatives, including Salmonella, Shigella, Neisseria, Pseudomonas (one of the few oral antipseudomonals).
Good intracellular penetration so active against organisms such as Chlamydia, Mycoplasma, Legionella and some Mycobacteria.
Good tissue penetration including central nervous system. 80% of orally administered drug is bioavailable so the IV route is only used when absorption impaired.
But no anti-anaerobic activity, and not very good against common gram positives eg Pneumococcus, Enterococcus, Staphylococcus (in fact, use is associated with MRSA). The newer types (Gatifloxacin, Moxifloxacin, Levofloxacin) have better gram positive activity but would still not be your first line choice, and have less anti-pseudomonal activity.
Not licensed under 1yr.
Only contraindication is previous tendon problem caused by it!
Adverse Effects:
Disabling, long-lasting (even irreversible) musculoskeletal and neurological problems reported, v rarely. So only use for severe infections, unless no other antibiotic appropriate. And stop ASAP if symptoms (muscle pain, joint pain, weakness, neuropathy etc)
Seizures (+/- predisposing condition)
Tendonitis – rupture can occur within 48hrs of starting, but can also be months later! Steroids at same time may increase risk, as may renal impairment and solid organ transplants
Arthropathy in immature animals – so avoided in children (except Nalidixic acid) unless extenuating circumstances (only reversible musculoskeletal symptoms have been reported). Arthropathy occurs in CF anyway.
Can prolong QT
Photosensitivity
Valve regurgitation – so caution if preceding valve disease or other risk factor eg connective tissue disorder (Ehlers-Danlos, Marfans), hypertension (!), Turners (!)
Talking here about type 1 IgE mediated wheat allergy. Not coeliac disease, which is an autoimmune process triggered by gluten.
Only 10% persists to adulthood, equivalent to milk/egg. Max IgE over 20 has median resolution age of 7, rises to 16 if max over 50. Unusually, IgE often remains positive even when tolerance has developed! But trend still useful for individual patient.
Wheat allergens – most commonly LMW glutenin, alpha and gamma gliadins, NOT omega. Technically gluten is found only in wheat, and is a complex of gliadin and other proteins, similar prolamins in other cereals have different names eg zein (rye), avenin (oat), hordein (barley)!
Level of omega 5 antibodies correlates with clinical severity of exercise induced anaphylaxis! Not specific though – Omega 5 antibodies are present in 80% with anaphylaxis to wheat (non-exercise induced) and 20-30% of wheat allergic with eczema. Useful for predicting anaphylaxis??
Note that those with grass pollen allergy often have non clinically significant IgE to wheat.
Lots of different names for wheat versions/products – Bulgar wheat, couscous, durum wheat, freekeh, einkorn, emmer, farola, kamut, malted wheat, semolina, spelt, triticale, wheat bran, wheat germ.
Presence of wheat starch in gluten free products (can be useful for producer) means the low level permitted for coeliac disease may still cause reactions if sufficient amount eaten, so avoid wheat based gluten free products if type 1 allergy.
But glutens present in non-wheat grains are not usually a problem for type 1 wheat allergy, so excessively restrictive to follow gluten free labels on things not made with wheat, eg oats!
Testing often suggests cross reactivity between different cereals but when you actually challenge, majority only react to one, and non wheat allergies pretty rare. Oat, rye, barley, maize allergy uncommon.
And strange how aeroallergy (to the pollen) so rarely translates to food allergy and vice versa.
[J ALLERGY CLIN IMMUNOL 1995;96:341-51]
So I would say no need to avoid or test unless symptomatic.
Cross contamination (as in coeliac) a big issue – crumbly! Toasters, butter, surfaces etc.
Hydrolysed vegetable protein sometimes comes from wheat, has to be declared as allergen but little evidence that it is still allergenic.
There are reports of allergy to deamidated wheat (“wheat protein isolate”), where tolerant to normal wheat. Found in cosmetics too.
Reintroduction
Typical ladders suggest starting with 1/2 teaspoon of Weetabix, toast, biscuit or pasta, doubling every 3 days if non type 1, more slowly if type 1.
Immunotherapy
There has been some work in the field of wheat immunotherapy.
2018 US multicentre RCT with “high protein vital wheat gluten flour” (n=46, median age 8.7 years) – initial escalation dosing first day from 0.1mg irradiated wheat powder (0.07mg protein; much more than wheat flour, which is only 7-16% protein) up to 12mg (8.5mg protein), escalation every 2 weeks to 1445 mg wheat protein (about half a slice?). Median threshold at start was 43mg protein.
Vial/capsule initially. Placebo subjects crossed-over to a high-dose-OIT, maximum 2748 mg wheat protein daily dose. Both regimes induced desensitization to 4443mg in the majority after 1 year of therapy – 52.2% (low dose OIT), 57.1% (high dose OIT). At 2 years, only 13% had sustained unresponsiveness (stopped wheat OIT for 8 –10 weeks). Adverse reactions were “comparable” with oral immunotherapy to other foods; 24% of the subjects discontinued the trial, predominantly due to gastrointestinal symptoms.
2020 Thai 3 step protocol found threshold dose of 20 mg of wheat protein. Starting dose of 1mg of wheat flour (0.1 mg of wheat protein) and increment every 30 minutes – starting OIT dose was then dose below threshold. Carrying medium used was cow or soy milk. Systemic reactions seen on 13 occasions in 26 patients; adrenaline used 6 times.
2021 Review here, and almost identical one here. Only one RCT!? Some studies used rush introduction, others clinic or even home updosing. Vital wheat probably more concentrated than regular wheat – so easier to hide in things?
Orzo pasta as more practical than flour!? 1 grain=5.2mg protein. Finnish study used cooked spaghetti in kids from age 6- one millimetre of cooked spaghetti = 0.3mg of wheat protein. 64% achieved target dose of 2g protein (24 strands!) within 4 months (first 5 weeks slow but then doubling every week, so pretty fast – only 10, 20, 40mm doses in clinic, others at home!) but almost half had to reduce dose during maintenance. Omega 5 gliadin only seemed to predict achieving target dose but lots of overlap. 12% used adrenaline at some point in 1yr trial. Reactions were frequent both during updosing and maintenance. Recommended against use of spaghetti in OIT!
But perhaps more measurement error/variation. Cooking time as factor? Richard Wasserman reports reactions to different wheat products when OIT done with crackers, so prefers Vital gluten (hard to dissolve… Either wait to dissolve itself (tedious) or shake vigorously in luke warm water).
Varying maintenance doses, from 53mg up to 5200mg (200g cooked noodles)!
It seems likely that sustained unresponsiveness is difficult to achieve.
Even in the highest dose trial, no patients required adrenaline during up-dosing and only one patient required it during home dosing. There is a concern about eosinophilic oesophagitis, as with other forms of food immunotherapy.
Exercise as a co-factor perhaps even more important for wheat – one small study showed that 10 minutes of running 30 minutes after wheat ingestion triggered a reaction in 67% of patients who had successfully achieved maintenance dose, and still an issue in half 5 years later. No obvious clinical predictors. Need an exercise provocation test before liberalizing exercise restrictions?
No obvious benefit from co-administering antihistamines and/or montelukast.
6yr follow up of low dose regimen still good results.
=allergic rhinoconjunctivitis due to seasonal triggers, typically grass and/or tree pollen, can also be weeds/moulds. First described by John Bostock in 1819, so a new disease!?
More likely if born in early months of year!?
So itchy, swollen, watery eyes, runny and/or blocked nose, sneezing. Often itchy throat and ears too. Cobble stone appearance can be seen at the back of throat.
Not dangerous, but can seriously affect quality of life: poor sleep, poor concentration (exams usually at worst time of year), embarrassment about snot. One study in England showed that children with hay fever requiring anti-histamines are significantly more likely (43%) not to achieve predicted exam grades, especially when using first generation sedating antihistamines such as Piriton (chlorphenamine) [Samantha Walker, JACI 2007: 120; 381-387].
Associated with other atopic conditions, such as food allergy and asthma. Moderate to severe hay fever also associated with worse, uncontrolled asthma. London study found hospital admissions for asthma 50% higher 3 days after high grass pollen levels (inconclusive for tree pollen). [Int J Biometeorol. 2017]Brussels study found similar, compounded by air pollution. Treatment of hay fever with intranasal steroids or class 2 antihistamines reduced admissions by up to 80%. [asthma res and pract2015]
Pollen is too large to trigger the lower airways directly, rather, pollen exposure in the upper airways trigger inflammation that travels down (probably over a period of weeks) to the lower airways. An exception is when pollen grains are fragmented, as seen in thunder storm asthma where one night in Melbourne, 2016, several thousand acute respiratory presentations came to ED (up over 600%), asthma admissions up over 900%, hospitals ran out of inhalers. 10 deaths implicated. [Australia, Clin Exp Allergy. 2018;48:1421‐1428]. Complex though, rain/moisture probably contribute to pollen grain rupture, and atmospherics bring surges of pollen down to ground level.
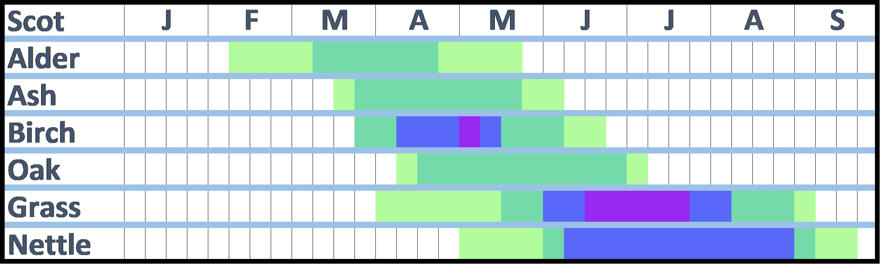
There are many different species of grass, but if allergic to one you tend to be allergic to all of them. Trees on the other hand vary, you tend to be allergic to specific groups of trees. In Europe the most important are birch (northern Europe) and olive (Southern Europe). Birch is related to alder, hazel, hornbeam, beech, oak, chestnut. Olive is related to ash. Weeds belong to various unrelated families.
Hazel trees can start producing pollen in January! Weeds such as nettle can continue producing pollen through September! Cypress blooms in winter!
Average start of grass season in Scotland is mid-May (dark green on chart below), high counts generally start 1st week of June (blue), peak (purple) is mid-June to mid-July. (Light green is earliest/latest appearance, low risk).
Average start of birch season in Scotland is last week in March, highest counts end April, early May.
It’s not just pollen count – the amount of allergen carried by the pollen (“pollen potency“) varies too. Correlates pretty closely but varies by time and place, 4-5 fold difference geographically (especially grass). France has the highest yearly average grass pollen potency, 7-fold higher than Portugal. Olive pollen from two locations 400km apart varied 4-fold in their allergen potency – in Portugal there are times when pollen from Spain probably more of a problem for triggering hay fever than pollen from “local” trees! [Health Impacts of Airborne Allergen Information Network (HIALINE project)]
Moulds seem more associated with asthma than hay fever.
Management
Watch the pollen count, and choose activities inside or outside accordingly. There are apps that can help with this. But note that the time of day is important too – for grass pollen, the risk is greatest in the first half of the morning and again from about 4pm in the afternoon, until late evening. But can persist into the early hours if temperatures remain high, this effect is particularly noticeable in the cities of the south of England. For tree pollen, the risk is usually during daylight hours only.
Closing windows, or at least not sitting near windows should help. Wash your hair more regularly. Don’t dry clothes outside. Pollen barrier balms available (evidence?). Big, wrap around sunglasses?
Air purifiers with a HEPA filter should help but doors and windows will need to be closed. Unfortunately the best ones tend to be big, expensive and noisy, and price does not mean good quality. Plus you have to remember to replace the filters. The cheapest Which? recommended one (the Electriq EAP500HC) costs over £200.
Choose when and where you are going on holiday carefully, so you get away during the worst period. North of Scotland and the islands have a short, late grass season (late June, early July). Coastal areas likely to be best (although often there are fields just back from the coast, so it may depend on the wind direction!). For tree pollen, season is earlier for most (see above), and there are parts of Scotland (Orkney, Lewis, Caithness, Sutherland) with very few trees. For holidays abroad, see World pollen data.
Medicines
Antihistamines – oral, nasal or eye drops. Various, some people find one works better than another Sedating antihistamines eg Chlorphenamine should be avoided except at night.
Cromoglycate eye drops are available, they work in a different way from antihistamines so may give additional benefit. But need to be given 4 times daily, which is inconvenient.
Nasal steroids useful if used correctly. Fluticasone is licensed from age 4 – Betnesol nasal drops from age 2 (but systemic absorption an issue). Combination steroid/antihistamine spray available from age 12.
Leukotriene receptor antagonist licensed for hay fever in children with asthma.
Short courses of oral steroids might be justified for special occasions.
Immunotherapy available. Grazax is sublingual grass product; Pollinex Grass and rye is subcutaneous. age not important cf ability to hold in mouth for 2 minutes! Metanalysis by Dhami S et al of grass desensitization in children, using either subcutaneous or sublingual therapy, found overall standardized mean difference (SMD) of -0.53 (95% CI -0.63, -0.42) in symptoms scores (roughly equal numbers of SCIT and SLIT studies, roughly equivalent scores) [Allergy 2017]. Deaths reported in asthmatics with poor control.
Itulazax is NICE approved tree pollen daily sublingual (need to start 16 weeks ahead of season, so last week in November; £80 on NHS). Pollinex tree is subcutaneous.
Licensed but none approved by SMC (Grazax rejected in 2008 and not re-submitted, Pollinex and Itulazax never submitted) for Scotland. Combined grass and house dust mite products?
Omalizumab – monoclonal anti-IgE – single injection of 300 mg omalizumab two weeks before start of the pollen season achieves better overall control of symptoms and QoL [adults, China 2022]. Evidence of benefit in allergic rhinitis with difficult asthma [adults, 3 years worth of monthly treatment, Italy 2020].
Group of nuts that includes hazelnut, almond, brazil nut, cashew, pecan, pistachio, walnut and macadamia. Definition of nut is actually a bit complicated, to do with whether the shell comes off spontaneously or not, but I stick to those defined by food labelling law.
Does not include peanut (a legume), coconut, pine nut, chestnut or tiger nut. You can be allergic to these as well, of course.
You can be allergic to just one, a couple or the whole lot. Risk of allergy to peanut is higher than if you weren’t allergic to anything.
Hazelnut and cashew allergies are common. Almond rare.
Cashew allergy goes with pistachio allergy (OR for being allergic to both 575). Cashew allergy is particularly associated with anaphylaxis, even more so than peanut (but less common as allergy and allergen so less well known). 3 components – Ana o1/2 are seed storage proteins. Ana o3 is a prolamin, and the component most likely to be associated with anaphylaxis, plus probably more useful for diagnosis than cashew IgE.
Pecan allergy goes with walnut allergy (OR 150).
Hazelnut goes with macadamia (OR 56.2) supposedly, although that’s not my experience.
One of the tree nuts. One of the most common food allergens in the UK. Adults seem to get less severe reactions than children. Anaphylaxis rare compared with peanut and other tree nuts.
Hazel tree is related to birch, and indeed hazelnut allergy can be associated with tree pollen allergy (hay fever and pollen food syndrome), as well as fruit allergies.
Cor a 1 is the least likely to cause systemic reactions, and then only with raw cf roast. But pretty much everyone tests positive for it, so not v helpful unless it is the only thing that is positive. You are usually also positive for rBet v 1/2, the birch pollen antigens.
Cor a 8/9/14 associated with systemic. Cor a 8 is LTP so likely fruit allergy too.
Cor a 9 and 14 (11s globulin and 2s albumin respectively, ie heat stable seed storage proteins) seem most useful for defining kids at risk of systemic reactions – >1kU/l and/or >5 respectively give specificity of >90% and sensitivity of 83% in kids for “allergy with objective symptoms” viz more than just a tingle/itch, so more likely to have severe reactions. That translates to a negative predictive value of about 93% (PPV not given). [Dutch study, JACI 2013;132(2):393]
German study found Cor a 14 had best AUC (0.89, cf 0.71 for whole hz). Level of 0.35 gave 85% sensitivity with 81% specificity. PPV doesn’t hit 90% until 47.8 though…
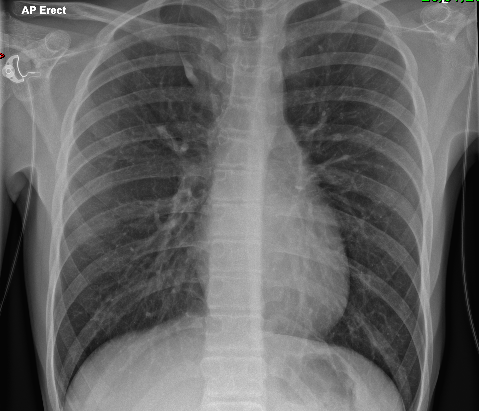
Start outside, work in – soft tissues, then bones, then lungs/heart, finally neck/infradiaphragmatic.
Safety check – position of lines/tunes, check apices for pneumothorax, any foreign bodies?
Adequacy
Rotation – look at symmetry of clavicles and anterior rib ends.
If clavicles high, then lordotic film. May obscure apices.
Penetration – should just be able to make out intravertebral spaces, without lung fields being too dark.
Inspiration – hila become artificially prominent if underinflated.
Thymus
Pesky thing! Can look like pneumonia. Latter more likely if air bronchograms, volume loss (displaced fissure/trachea/mediastinum), effusion. Classically:
indentations where ribs overlie.
Pointy outside edge (“sail sign”).
No mass effect
Lowish density – should still be able to see vascular markings of lung behind
Spinnaker sign is where pneumomediastinum around thymus creates long curving line.
Other normal things
Azygos lobe – normal variant where RUL has near vertical line curving up and out, from thick point (anomalous azygous vein) – giving impression of mediastinal mass.
Azygos lobe at upper right
Mach effect – a line parallel to heart border, looks like pneumocardium but actually optical illusion where your eye “detects” border where there isn’t one…
One diaphragm usually higher than other – both ok, as long as no more than 2cm (one rib space).
Other
Hilum – rings or tram lines suggest bronchitis. Round opacity adjacent to and larger than ring suggests vascular prominence due to left to right shunt.
Silhouette sign – where heart border and/or diaphragm obscured in lower zone due to consolidation in lower lobe (left or right).
Effusion – vertical line at costophrenic angle.
Round pneumonia – will have air bronchograms, compare mass.
Collapse vs consolidation – sharp lower border is the fissure so if deviated then collapse.
Pneumothorax – lucency without clear edge may suggest lung hyperinflation eg bronchial atresia.
If edge projects below diaphragm then likely to be skin fold!
Foreign body – get expiratory film, which will enhance air trapping.
Amino acid homocysteine is converted to methionine (“remethylated”) – cobalamin is involved in some of these processes, folate metabolism also important.
Various disorders.
Variety of presentations, at different ages:
Neurological (central and peripheral)
Feeding difficulties, apnoea in babies
Seizures
Subacute combined degeneration of spinal cord (peripheral neuropathy, ataxia, incontinence)
Start intramuscular B12 (hydroxocobalamin) as soon as samples collected, to prevent end organ damage.
Betaine should be started if high homocysteine with low methionine found, helps push conversion to methionine.
Homocystinuria
Autosomal recessive condition of high homocysteine in blood and urine, causing similar neurological problems, thrombosis, Marfanoid appearance, downward subluxing lenses.
Getting it right for every child. A framework for dealing with children and young people, looking at a range of values (SHANARRI).
Children and Young People (Scotland) Act 2014 made provision for Named Person and Child’s plan, but after review in 2019, amid privacy concerns (brought by Christian Institute, among others), government decided not to pursue legislation. Supreme court found that “duty to share information”, although well intentioned, was potentially at odds with article 8 of European convention on Human rights (“Privacy and family life”).