See also antipyretic treatment.
Fascinating how fever affects parents! Fever phobia first described in the literature in 1980 by Schmidtt. Found in many different cultures and countries, not related simply to child mortality rates or education. And does not appear to be declining over time. Also commonly found in health care professionals esp nurses.
Interesting cultural variation eg Hispanic Americans vs white, Bedouin vs Jewish Israelis.
The main fears for parents are seizures, brain damage, dehydration, whereas the issue for health care is the potential for underlying, serious illness, typically bacterial eg meningitis, pneumonia, septicaemia etc.
Hyperthermia, ie unregulated rise in temperature (think dogs in cars) is dangerous, causes brain damage. Hyperpyrexia on the other hand, where body “thermostat” reset, is not dangerous. It can precipitate febrile convulsions, but only really in children with a genetic susceptibility or at least an underlying predisposition to seizures.
In a qualitative study of Dutch parents, it was clear that when parents did not feel recognised in their concern or felt criticised, anxiety increased as well as the threshold to seek healthcare for future illnesses. The authors recommend that health care professionals recognise parental intuition and provide clear information on alarming signs and potential diagnoses to empower parents [BMJ Open 2018;8:e021697].
Measuring/Detecting
Touch is sensitive (90%) but not specific (50%) for fever – so don’t dismiss parental reporting entirely. [J Trop Pediatr. 2008 Feb;54(1):70-3 PMID 18039678]
NICE recommends digital thermometer in axilla, else tympanic thermometer or chemical dot thermometer in axilla (still not great cf rectal, particularly when parents doing it with over the counter devices cf nurses with hospital equipment [BMC Fam Pract. 2005; 6: 3]).
Over the counter devices sadly provide little useful practical information to parents – in fact most do not even give correct criteria for pyrexia and few give useful advice on managing fever [Br J Gen Pract. 2015 Jun; 65(635): e366–e371.]
Assessment
The height of fever is associated with bacterial, rather than viral infection, but only over 40 degrees: in hyperpyrexia (> 41.1.degC) still only 20% will have serious bacterial infection so really not v helpful. Chronic underlying illness, prematurity or diarrhoea increase the risk of a bacterial cause, rhinorrhoea or other viral symptom decreases it. Age, maximum temperature, and total white blood cell count were surprisingly not predictive of either bacterial or viral illness! (n=103). (Pediatrics. 118(1):34-40, 2006 PMID 16818546)
Red flags:
- Cold limbs – sepsis
- Leg pains, thirst – sepsis esp meningococcal
- Short history – meningococcal
- Disproportionate heart rate – sepsis
- Foreign travel
- Unimmunised – Pneumococcal, Hib
- Prematurity, chronic disease
History of fever at home, compared with actual fever on admission, is lower risk (RR 0.68) but not enough to ignore [Journal of Pediatrics. 204:191-195, 2019 01.PMID 30291019].
Fever without source causes concern, although generally it will either become more obvious where the source is or else it will sort itself out. Only when fever has been persistent for more than 7 days in a child in whom a careful thorough history and physical examination, and preliminary laboratory data fail to reveal a probable cause for the fever, can you reasonably start talking about a pyrexia of unknown origin (PUO)!.
The risk of invasive bacterial disease in young children with unexplained fever presenting to hospital has certainly declined with modern immunisation schedules so difficult to compare with historical data.
NICE published a Traffic Light system for detecting serious illness in febrile under 5s. A bit unwieldy, seems to cover the main issues, retrospectively sensitivity is only about 85%, and specificity only 29% for serious bacterial infection.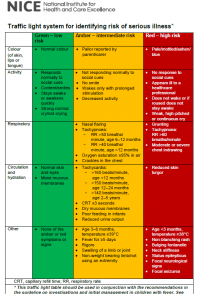
Red symptoms/signs are ones that clearly indicate serious illness eg
- weak, high pitched or continuous cry (meningitis)
- grunting
- tachypnoea >60
- reduced skin turgor
The Amber group includes the vast majority of children coming to hospital with fever. In particular:
- creps
- tachypnoea >50 (under 1) or >40 over 1
- tachycardia >160 (under 1), >150 (1-2), >140 (over 2)
- rigors (not probably much more predictive than high fever – ?higher risk of urinary sepsis?)
And anyway, we know signs and symptoms other than classic neck stiffness etc fail to predict outcome; best predictor is still “something is wrong” or “appears unwell”. In Jonathan Craig’s big Australian study looking at more than 25 clinical indicators for bacteraemia, UTI and pneumonia, “appearing generally unwell” was the strongest diagnostic marker for all 3 groups. Raised temperature, no fluid intake in the previous 24 hours, increased capillary refill time, and chronic disease also predictive. [BMJ 2010;340:c1594]
Hence most important primary care action is prompt clinical assessment by experienced clinician. [BrJGP 2007;57:538, pmid 17727746]
Under 3 months – if previously healthy, no evidence of focus, normal WCC then risk is minimal. Procalcitonin appears to be best performing test but not widely available. American Academy of Pediatrics recommends fever (38.5), neutrophil count (5.2) and CRP (20) as cut offs for low risk otherwise. US audit of 1000 infants found this meant 45% of cases could be treated as low risk, with 100% sensitivity and specificity for bacteraemia (but 93.7% NPV for UTI).[Brett Burstein, Montreal 2022]
Ambulatory care suggested by Dagan back in 1988 (J ped 112). Remember that if fever has been of short duration eg under 12 hrs, inflammatory markers become less reliable. [Pratt, Peds International 2007 PMID 17250502]
Baraff recommends that all febrile neonates get full sepsis screen including LP. Between 1 and 3 months of age the rate of serious bacterial infection is much lower – if non-toxic looking (see below), use inflammatory markers only.
People continue to look at risk factors – with COVID perhaps things different again.
Over 3 months – historically fever greater than 39 predicted bacteraemia in 3% of kids (before conj pneumococcal vaccine) – but was often transient even without antibiotics!
NB even if a risk falls to 1%, the cumulative chance of getting at least 1 wrong after 100 patients rises to 50%!
Compared with other scoring systems, NICE traffic lights work pretty well but note how none of these systems work as well as they were supposed to, and performance varies across different datasets.
Adding urinalysis improved sensitivity to 92%, since most of the missed infections were UTI. (De et al, BMJ 346: f866 ). Thus, prize winning haiku:
Improve the NICE guide
for under 5s with fever
Urinalysis
See also antipyretic treatment.