Only need fixed if persist after first year of life or develop later in childhood, as regression of processus is less likely to occur.
Category Archives: General paediatrics
Kawasaki syndrome
A syndrome of unknown cause, characterised by persistent fever, conjunctivitis and mucosal changes eg strawberry tongue in a young child who has often been treated empirically with antibiotics without improvement, and is invariably miserable. Potentially complicated by coronary aneurysms, which may be fatal. Kawasaki’s is the leading cause of acquired heart disease globally after rheumatic fever, and is the leading cause in the North.
It is a vasculitis affecting medium sized arteries, and other arterial vessels down to capillary size. Second most common vasculitis in childhood, after IgA vasculitis.
Was thought to be a superantigen disorder, ie with no specific infectious agent, polyclonal B activation – coronary aneurysms have been seen in other superantigen diseases eg toxic shock, have also been reported in meningococcal septicaemia. But now thought to be conventional, but unknown, infectious trigger.
Similarities with COVID PIMS-TS.
Genetics important, risk higher in East Asian immigrants, plus family history, single nucelotide polymorphisms found in 6 genes including FcγR2a, caspase 3 (CASP3), and human leukocyte antigen class II.
Clustering has been shown (Knox test significant within the space-time interval of 3 km and 3-5 days) which suggests an infectious trigger [PIDJ 27(11):981-985, Nov 2008]. TNF alpha seems important, in an animal model, knock out mice or anti TNF treatment prevents aneurysm development.
The underlying pathology is a vasculitis, and although coronary disease is the best recognized there is increasing evidence that other medium sized arteries are affected with descriptions in the literature of peripheral gangrene and cerebral infarction. Proposed model includes necrotizing vasculitis, plus chronic/subacute vasculitis, 2 weeks after onset and sometimes lasting months, with a unique type of luminal myofibroblastic proliferation.
Epidemiology
More common in males, peak age 18-24 months.
BPSU Kawasaki – 553 cases were notified: 389 had complete KD, 46 had atypical KD and 116 had incomplete KD! Median time to IVIG in those with Coronary artery aneurysms (CAAs) was 10 days cf 7 days for those without. Rate of CAA in under 1yr was 39%. 19% overall had CAA despite treatment. Associated with low albumin, and incomplete. Only 1.6% developed giant aneurysms, which have the worst prognosis, of course.
Risk of CAA estimated at 20-40% if untreated. [Archives PMID 30104394]
Incidence in west seems to have plateaued, after decades of increase (?ascertainment bias). 10-20x higher rate in NE Asia (Japan, Taiwan, Korea), plus continues to increase! 1% of all Japanese kids will have had KD by age 10. But unrecognized before 1950, whereas pathological specimens in UK from over a 100yrs ago show same process.
Less complications in Asia! Better diagnosis? Arguably all European cases could be considered high risk…
Japan has had 3 epidemics, the only country to have had them, but none since 1986.
Data from China and India indicate increase, with only a few case reports prior to 1990. Rate in Chandigarh equivalent to UK now, presumably underestimate, but already outnumbers rheumatic fever cases. Also high rate in Kerala, but related to affluence or health care availability? Rate in Shanghai approaching NE Asia rate. Rate in Hong Kong has tripled in 20 years. Will become the predominant cause of acquired cardiac disease?
Association between seasonal wind patterns in Pacific and KD rates in Japan, California and Hawaii! May relate to infectious agents.
[Singh S, et al. Arch Dis Child 2015;100:1084–1088. doi:10.1136/archdischild-2014-307536]
Case definition
(American Heart Association):
- Fever of 5 days duration or more
- plus 4 of the following (ie only drop 1):
- Conjunctivitis: Bilateral, bulbar, without exudate
- Lymphadenopathy: Cervical, >1.5 cm
- Rash: Polymorphous, no vesicles or crusts
- Changes of lips or oral mucosa: Red cracked lips; “strawberry” tongue; or diffuse erythema of oropharynx
- Changes of extremities:
- Initial stage, erythema and oedema of palms and soles
- Convalescent stage (about two weeks) periungual desquamation of fingers and toes

These are all acute febrile stage symptoms, first 2 weeks (besides the desquamation) – but not necessarily all at the same time, sometimes only on history. After 2 weeks, persistent irritability, poor appetite, conjunctival injection. If still febrile at this point then high risk of cardiac complications. Any coronary artery ectasia or aneurysms may enlarge from week 4-8. Ectasia may resolve.
In Japan, prolonged fever is one of the optional features – 1/3 of Japanese children get IVIG before day 4! McCrindle guideline (AHA, 2017) suggests complete Kawasaki disease may be diagnosed with 4 days (possibly even 3 days) fever if one of the features is peripheral erythema/swelling.
Many people would also diagnose if only 3 of these features plus coronary artery aneurysms detected. Lymphadenopathy is the least common feature (?easy to miss) – esp uncommon in younger children. Perineal desquamation is also quite characteristic.
There may also be abdominal pain, diarrhoea, hepatitis/pancreatitis, arthralgia/arthritis, aseptic meningitis, facial nerve palsy and pneumonitis (with or without pulmonary nodules). There may be a murmur (mitral incompetence), and myocarditis can occur but it is rarely severe. CXR changes (nodules, peribronchial and interstitial infiltrates). Aortic root enlargement. Desquamation in groin. Hydrocoele and gall bladder hydrops! Anterior uveitis. Renal involvement, encephalopathy have been described, macrophage activation syndrome has been reported rarely.
Pitfalls –
- infants, adolescents (“glandular fever”).
- Signs change over time – rash fades, desquamates, then nail changes but similarly lymph nodes, mouth changes. So at any one time only a few features may be evident – especially beyond first week.
- Normal or low platelets (actually a high risk feature in some scoring systems)
- Sterile pyuria (“UTI”), “aseptic meningitis”
- Presentations with myocarditis, surgical abdomen (GI vasculitis)
- Single dose of IVIG without response does not mean diagnosis is wrong, in fact means more aggressive treatment required.
- Beware positive cultures putting you off diagnosis! Might be triggering infection! Even Strep, adenovirus
Tips –
- BCG reactivation as a clue
- Arthritis as a clue
- Axillary/inguinal aneurysms on examination? [Janet G-M]
- Repeat echo early, especially where diagnosis still not clear cut. Cardiology need chasing!?
- IVIG raises ESR! Don’t interpret as treatment failure!
- Incomplete/uncertain have highest risk of complications! So consider if fever >=5/7 with 2 criteria, or infants [only infants?] with fever >= 7/7 without necessarily any criteria, but no other explanation! CRP>30 and ESR>40 should trigger further assessment eg echo and use of additional lab criteria eg anaemia, high platelets (>450 beyond day 7, but also <140), high ALT, high WCC (>15), low albumin (<30) . Echo if CRP/ESR low but peeling. 3 or more additional lab criteria sufficient to make diagnosis.
Many of the clinical features of the disease are outbreak dependent with a different spectrum of clinical findings in one mini-outbreak compared with another, and with cases having similar clinical phenotypes clustering temporally.
So consider echo in any young child with persistent fever.
The term atypical or incomplete Kawasaki disease is used for cases without the required number of features. Whether this is the same disease or not is unclear; there will undoubtedly be some cases that overlap with other systemic vasculitides eg polyarteritis nodosa (PAN). In PAN, mucocutaneous changes are uncommon, whereas renal disease is common. Gall bladder hydrops appears to be unique to Kawasaki’s. On the other hand, having a rigid case definition is perhaps unhelpful since incomplete cases are often seen, particularly in infants, and are associated with a delay in diagnosis and worse prognosis. Under the age of 3 months, the majority of cases with coronary aneurysms have atypical presentations.
McCrindle AHA guideline suggest incomplete KD should be diagnosed where:
Differential diagnosis
- Scarlet fever
- Toxic shock syndrome – some cases of “Kawasaki shock syndrome” have been described
- Scalded skin syndrome
- Measles
- Drug reaction incl Steven-Johnson syndrome
- Rickettsial infection eg Rocky Mountain spotted fever
- Systemic onset juvenile idiopathic arthritis
- Leptospirosis
- PIMS/TS
- Other vasculitis eg PAN, Wegener.
Investigations mainly help exclude alternative diagnoses. Infection may have triggered KD so may need to treat for both – antibiotics if concern – get cultures. Typically with the disease itself test results simply indicate systemic inflammation and can be useful for monitoring response to treatment. Hence there are usually elevated white cells, platelets, ESR and CRP, ferritin/coag (MAS?), troponin (myocardial involvement?), D-dimers, LDH. Liver function tests are often mildly deranged. Low sodium and albumin suggest vascular leak. The ECG may have PR interval changes, and ST segment or T wave changes. Echocardiography (ideally within 2 weeks of onset of fever but as soon as possible) may reveal dilated, ectatic coronary arteries or frank aneurysms.
Consider CXR, Abdo USS (incl gall bladder).
Treatment
SPARN 2024 guidelines (based on AHA) advises taking serum for storage if possible, prior to IVIG. Refer for echo within 1-2 days assuming normal ECG and CXR. Admit under Infectious diseases or Rheumatology unless cardiomegaly, abnormal ECG, heart failure or giant aneurysms.
As with Eleftheriou (2013) guidelines, methylprednisolone in addition to IVIG/aspirin if high risk viz infants, severe inflammation (CRP>100, liver dysfunction, hypoalbuminaemia, anaemia), shock or HLH, evolving anuerysms/ectasia, failed IVIG – consider if thrombocytopaenia, late presentation). Infliximab is included as an option for resistant or recrudescent disease. Of course, diagnosis should be reconsidered if response to treatment is poor.
Standard treatment is with intravenous immunoglobulin (IVIG) 2g/kg over 12 hours, ideally within the first 7-10 days of the illness, and with aspirin (high initial dose 30-50 mg/kg/day in 4 divided doses orally during the acute phase – AHA still recommends before switching to low dose but insufficient evidence of benefit). This combination reduces the risk of aneurysm formation from 25% to 9%. Most will respond to a single dose, but about 20% will require a second dose. Add steroids if not given already and consider second dose if persistent fever and/or failure of CRP to fall at least 50% within 48 hours. Of these, only a half will then defervesce.
IVIG side effects – fever, headache, joint pain, aseptic meningitis, BBV, allergic reaction (?), raised ESR. Remember to defer immunisations for 3 months.
Once defervescence has occurred, the aspirin dose can be reduced to an anti-platelet dose of 3-5mg/kg/day (max 75mg). Aspirin is stopped after 6 weeks unless aneurysms found.
Duration of fever is the most powerful predictor of poor coronary outcome (one additional day of fever increasing the odds of aneurysm development by 3-5x). Delayed diagnosis is usually a reflection of slow evolution of criteria rather than atypical presentation – in that study, diagnosis after 10 days had a 2.8x higher risk of aneurysms (although they also had higher platelet counts). [Pediatrics. 115(4):e428-33, 2005. PMID 15805345]
Methylprednisolone treatment is 0.8mg/kg BD IV for 5-7 day or until CRP normal, followed by Prednisolone 2mg/kg weaning over 2-3 weeks. Other regimes are Methylpred 10-30mg/kg IV OD for 3 days followed by prednisolone.
In Europe steroids reserved for worse cases – but by epidemiology, all European cases could be considered high risk?? 39% of under 1yrs had coronary aneurysms (BPSU study). Europe Kawasaki trial in progress (KDCAAP) – Adding immediate corticosteroid treatment to standard of care IVIG and aspirin.
Scoring
Several scorings systems have been developed to predict IVIG resistance and poor outcome. Kobayashi criteria used to predict IVIG failure (5+ points), but more sensitive in Japanese populations – just 33% in Non-Japanese, with 87% specificity:
- Age<12 months (2 points)
- Fever <=4 days (1 point)
- Na<=133 (2 points)
- ALT>=100 (1 point)
- Plts <300 (1 point)
- CRP>10 (1 point)
- >80% neutrophils (2 points)
Echo
ECG and echo should be done as soon as possible but should not delay treatment. Urgent if heart failure, cardiomegaly on CXR or ECG abnormalities. If first echo is normal and CRP normal after 1 week, repeat scans recommended at 2 and 6-8 weeks. But chase cardiology to repeat early if diagnosis unclear.
Those with Z score more than 10 (“large”) have 25% risk of coronary event within 10yrs (girls), 50% (boys)!
Most aneurysms will resolve over time, unless they are giant (>8mm). Serial echocardiography should be done to monitor resolution. Evidence of subacute chronic vasculitis for months (post-mortem cases) so move now to infliximab treatment etc after initial immunosuppression.
Warfarin should be considered for giant aneurysms, with initial heparinization to prevent paradoxical thrombosis, although its potential for complications in young children is significant. Stress testing and angiography may be appropriate. Aspirin can be discontinued if aneurysms resolve, but it is likely that the atherosclerosis risk remains high and life long follow up to address other risk factors is sensible.
Mortality in the UK has been as high as 3.7%, but is much lower in Japan.
[2020 ArchDisChild Ed and Practice Kelly] [2017 AHA guidelines][Eleftheriou Arch Dis Child 2014;99:74–83, J Paed and Child Health 49 (2013) 614–623]
Premature atrial extrasystoles
PACs for short. 
So you get extra atrial beats, from somewhere in the atria outside the SA node. The P waves therefore look odd, esp if they fall on top of a T wave. They can even be upside down if close to the AV node, the depolarisation is therefore in reverse and the PR interval is abnormally short. You usually do get a QRS after but sometimes it is blocked completely, and sometimes you get a RBBB pattern (RBBB has a longer refractory period).
You usually get a compensatory pause as the SA node is reset.
So the patient may feel a fast, extra beat, then a skip.
Considered normal! Can be very frequent eg bigeminy (every other beat is a PAC), and you can get runs (“couplets”). But if you have an abnormal heart already eg WPW, then it may be a trigger for a re-entrant tachycardia.
UK vaccine schedule
Changes depending on availability (and cost) of new vaccines, changes in epidemiology. And levels of public acceptance! Recommendations made by JCVI (Joint committee on vaccines and immunization). Most recent change is introduction of MenB (Bexsero).
- At, 2, 3 and 4 months, a 5 in 1 vaccine containing diphtheria/tetanus/pertussis with polio and Hib is given (Pediacel).
- Prevnar (pneumococcal conjugate, PCV-13) is given at 2 and 4 months with a booster at 12-13 months
- MenC now given at 3 months only (other 2 doses dropped), in between Prevnar, with a booster at MMR time.
- Oral rotavirus vaccine is now given at 2 and 3 months.
- Bexsero (MenB) vaccine is given at 2 and 4 months, with booster at 12-13 months.
At 12-13 months, MMR – along with boosters of Hib/MenC (Menitorix), Prevnar and MenB
Annual nasal influenza vaccines are being phased in over next few years, currently all primary school and ages 2-4yrs. Will eventually be all up to 16.
At 3yrs 4 months- 5yrs, preschool booster – DTP/Polio (Repevax, no Hib) and MMR again.
At 13yrs, BCG has been dropped as a universal vaccine. There is now a booster of MenC, along with Tetanus, diphtheria (low dose) and polio (no pertussis, Revaxis).
Girls between 12 and 14yrs get 2 doses of HPV vaccine, at least 6/12 apart.
Over 65s get scheduled PPV (pneumococcal polysaccharide, once) and annual influenza.
Over 70s get a single Shingles vaccine.
The acellular pertussis vaccine (3 or 5 antigens cf 3000 in whole cell) is associated with less reactions (but less effective and immunity shorter lasting); IPV (injectable) polio vaccine has same efficacy as OPV (oral, live, Sabin, herd immunity), plus no vaccine associated disease.
These newer vaccines have fewer reactions, and do not contain thiomersal. Not that there’s any evidence against mercury, but plan to eliminate it has been in place for several years.
There was also an issue with loss of Hib efficacy when using 3 in 1 DTP for primary immunizations, which is not seen with Pediacel.
No individual boosters for tetanus are available. Choice is between Infanrix (DTaP), Repevax or Revaxis.
Instead of BCG for all adolescents, risk factor approach introduced: BCG will be offered to all infants in health boards with incidence over 40/10 000 (none in Scotland), and to those with parent or grandparent from high incidence area.
Rhinitis QOL
You can just use generic SF-36 questionnaire, statistically significant differences between patients and controls were observed in seven of nine dimensions in the SF-36 questionnaire. Or RQLQ score (mini-form also available). (J Allergy Clin Immunol 1997;99:S815-9.) SF-36 particuarly highlights mental adverse effects, RQLQ highlights sleep disturbance.
Quality-of-life parameters measured by the RQLQ questionnaire:
- Sleep – Lack of a good night’s sleep, Wake during the night, Difficulty getting to sleep
- Non-hay-fever symptoms – Tiredness, Fatigue, Worn out, Reduced productivity, Poor concentration, Thirst, Headache
- Practical problems -Need to blow nose repeatedly,Need to rub nose/eyes,Inconvenience of having to carry tissues or handkerchief
- Nasal symptoms -Stuffy/blocked,Sneezing,Runny,Itchy
- Eye symptoms – Itchy, Watery, Swollen, Sore
- Emotions – Irritable, Frustrated, Impatient or restless, Embarrassed by nose/eye symptoms
- Activities eg Bicycling Cooking Dancing Doing home maintenance Doing housework Gardening Eating out Jogging, exercising, or running Attending public events Driving a car Watching TV or a movie Singing Mowing the lawn Playing with pets Doing regular social activities Talking (public speaking) Studying or doing homework Taking a test or quiz Visiting friends or relatives Going for a walk Having sexual intercourse Carrying out activities at work Reading Playing sports
Juniper and Guyatt
Bruising
Typical areas of accidental bruising:

Typical pattern of abusive bruising:
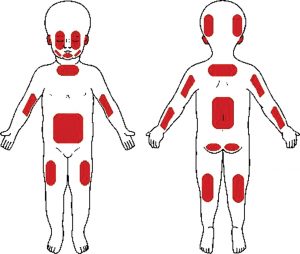
From prospective longitudinal study of children (<6 years):
- 6.7% of premobile children had at least one bruise (2.2% of babies who could not roll over and 9.8% in those who could)
- Most common site affected in all groups was below the knees, followed by ‘facial T’ and head in premobile and early mobile.
- The ears, neck, buttocks, genitalia and hands were rarely bruised (<1%).
- Gender, season or the level of social deprivation not associated with bruising patterns, although having a sibling increased the mean number of bruises.
- There was considerable variation in the number of bruises recorded between different children, which increased with developmental stage, and was greater than the variation between numbers of bruises in collections from the same child over time – so some kids do just bruise more than others?
Differential
Are you sure it isn’t a Mongolian blue spot? Or capillary haemangioma? Or erythema nodosum?
Cupping in Chinese culture! Dermatitis artefacta?
- Thrombocytopenia. Note film can show clues – inclusion granules in Chediak-Higashi.
- Factor deficiency – bleeding from umbilical stump classic for XIII deficiency. Girls can have bleeding problems even if carriers rather than completely factor deficient.
- Glanzmann’s thrombasthenia – platelet count normal! But severe eg fingertip bruising and bleeding from vaccination sites. Other platelet defects similarly.
History
Haematomas after Vit K at birth or immunisations? Bleeding from umbilical stump or Guthrie test? Dental treatment? Joint swelling or pseudoparalysis that might suggest a haemarthrosis?
Family history? 30% of haemophilias de novo mutations.
Skin/joint hypermobility/elasticity? See Ehlers-Danlos.
Listeria
An intracellular gram positive rod – not many of those, apart from in probiotic drinks! Resistant to cold and salt, so particularly a problem in ready to eat foods eg deli meats, hot dogs (unless steaming hot), cheese esp soft (incl blue veined, but excl mozzarella), raw and cooked poultry, ice cream, raw vegetables, raw and smoked fish (unless in shelf stable form). Melons and hummus have been sources in US. In adults, tends to affect those with underlying health problems.
Infection in pregnancy often undiagnosed. May cause preterm labour or intrauterine death. Infection at birth may be severe, with classic fine papular rash, widespread microabscesses and granulomas, and bacteria visible on gram stain of the meconium. Or infection may be late in onset eg 1-2 weeks, with meningitis (note low counts cf other causes), else endocarditis, osteomyelitis etc.
Preterm meconium staining of the amniotic fluid (MSAF) is a “classic” feature – was observed in 4.3% of infants below 33/40. No maternal or infant listeriosis was identified in any of the 1000 cases. MSAF was associated with prolonged rupture of the membranes and severe (grade 3/4) intraventricular haemorrhage (OR 2), not sepsis or mortality. (Simpsons, Arch Dis Child Fet 2004)
Surveillance study of bacterial meningitis in infants aged <90 days in the UK 2010-11 showed that then usual three bacteria (GBS, E. Coli and Listeria) remained dominant, their frequency varied significantly by month of life. In the first 30 days of life. L. monocytogenes was the third most common bacteria, responsible for 6% of cases. The median age of meningitis due to L. monocytogenes was 13 days (IQR 3–18 days) with the oldest infant being 29 days; Listeria meningitis was therefore not seen beyond the 1st month of life. Of the 11 cases of Listeria meningitis, a good number (although a minority) were preterm and most first became unwell when at home. 2 cases had serious complications but no deaths.
Public Health England have published 24 years data on listeria septicaemia and meningitis. 97% of all cases presented in the first 30 days of life. Bacteraemia is more common but tends to be early onset (<7 days of age) whereas most meningitis were late onset.
It is also prudent to consider the possibility of Listeria infection in older infants (and therefore add amoxicillin) if:
- Gram-positive rods are seen in the cerebrospinal fluid,
- if the infant is immunocompromised
- or if the clinical response to empirical therapy is suboptimal
Treat with high dose amoxicillin/ampicillin. Gentamicin is synergistic but does not penetrate intracellular compartment (or CSF) – can be stopped after a week assuming good clinical improvement. For allergic, TMP-SMX (Septrin) is best alternative! Cephalosporins are useless! Treat for 2 weeks if no meningitis, at least 3 weeks if meningitis, longer if abscesses or heart involvement.
[Okike, Arch Dis Child 2015;100:426-431]
Hepatitis B
Highly infectious blood borne virus. A single contaminated needle stick injury carries a significant risk of transmission. In endemic areas, significant rates of postnatal infection in children, presumably from minor trauma.
Acute infection develops over 1-6 weeks and can be fulminant. Symptoms are non-specific fever, lethargy, abdo pain. 15% have serum sickness type symptoms in pre-icteric phase viz fever, arthralgia, urticaria. Jaundice then develops. Various antigens, which may or may not clear as antibodies produced, used to diagnose, judge stage of infection, and infectivity.
- HBsAg – shows Acute or chronic hepatitis B infection. Can be negative in acute fulminant disease.
- Anti HBs (or Anti HBs) – Immunity to hepatitis B, postinfective (only 6% of patients) or with active or passive immunization
- Anti HBc IgM – first antibody to appear, even before HBsAg. High titer: acute hepatitis; Low titer: chronic infection
- Anti HBc IgG – Past exposure to hepatitis B, or maternal antibody crossing placenta in young infants
- HBeAg – highly infectious. Without treatment, 85% of children clear HBe.
- anti HBe – not immune, but low infectivity. Do not develop chronic hepatitis; but low risk of hepatocellular carcinoma persists.
NB there may be an interval following the disappearance of a hep B antigen before its antibody becomes detectable.
For acute hepatitis, no specific treatment is required, just supportive. If fulminant, some people use antivirals, but basically the issue is whether you need to transplant – see below.
Carrier rate (ie chronic infection, = HBsAg pos for 6/12, and hence potential for serious sequelae) is higher in males and greatest in those infected in first 3 years of life. Also higher in those with mild symptoms viz anicteric with minimal elevation of transaminases.
Some carriers will be inactive with anti-HBe, low levels of DNA (<100 000 copies on PCR) and normal transaminases. Liver disease progresses very slowly if at all, although hepatocellular carcinoma risk is still higher than normal (but much less than in HbeAg positive). Monitor LFTs every 6-12 months.
In active chronic infection, DNA levels are high indicating active replication, transaminases are 2x the upper limit of normal or higher, and biopsy will show stage 4 histological activity or more. HBeAg is usually positive although some mutants will be negative. Adults with chronic hep B have 20% cirrhosis rate after 10 years and 37% after 15 years. Alcohol intake is an independent factor. Hepatocellular Ca rate is about half that.
When to biopsy is tricky, partly because the clinical course is unpredictable but also because treatment is ineffective. Transaminases can be raised transiently, so repeat after 1-3 months. Histological cirrhosis has a poor prognosis. With treatment, 32% of patients with chronic disease clear HBeAg cf 11% of untreated (metanalysis). There is no benefit in patients with normal LFTs.
Do USS and alpha fetoprotein every 2 years as screening for hepatocellular Ca for both inactive carriers and chronically infected.
Other management points –
- immunisation of household contacts
- vaccination against hepatitis A (in low prevalence areas)
- avoiding alcohol
- safe sexual practices
- weight reduction
- Careers advice
- Immunosuppressive drugs may activate hepatitis B infection. Equally, immunosuppressed children may have hepatitis B infection without serological evidence – so do PCR.
Treatment
For acute, no specific treatment, just supportive. If fulminant, look for co-infections that may have precipitated episode. Main issue is whether transplant required, although American Association for study of liver diseases recommends using antivirals in adults: no great evidence but seem reasonably safe, and reduces risk of re-infection of grafted liver after transplant (pretty inevitable – HBIg post transplant also delays infection but resistant mutants come through). Lamivudine or telbivudine suggested when the anticipated duration of treatment is short; otherwise, entecavir is preferred. Treat until HBsAg cleared or indefinitely in transplants. Interferon is contraindiated.
For chronic infection:
- Pegylated IFN alpha (5 million units a day or 10 MU thrice SC for 48 weeks) both antiviral and immunomodulatory activity.
Other issues:
- Co-infection with HCV has a poorer prognosis even though DNA levels may be less; treatment should be considered at 1000+ copies.
- In decompensated cirrhosis, transplantation is the only definitely effective option. Lamivudine may help (historical controls). IFN increases complications.
Hepatitis A
Faeco-oral transmission. Global distribution.
Incubation 4/52, can be asymptomatic in young children. Non-specific fever, malaise, possibly RUQ pain before jaundice appears, usually with rapid relief in symptoms. Up to 1% however have fulminant disease with hepatic failure.
Post exposure prophylaxis for hepatitis A with hepatitis A vaccine reduces secondary infection rate from 13% to 2.8% (NNT=18).
See also viral hepatitis.
Viral hepatitis
- Hepatitis A virus
- Hepatitis B virus
- Hepatitis C virus
Plus the newer D (faeco-oral as A, particularly severe in pregnant women) and E (a co-factor in Hepatitis B infection).
But a range of other viruses can cause hepatitis eg EBV, Varicella.